


LENSES & MPS
Contact Lens-Associated Infiltrative Keratitis and Multipurpose Solutions
This article looks at a private practice's experience with CLAIK and silicone hydrogel wear in 2010.
By Andrew J. Sacco, OD, FAAO
Superior oxygen transmissibility, outstanding comfort, and affordable prices make silicone hydrogel (SiHy) lenses a first choice among many practitioners. In 2010, SiHy materials accounted for 73 percent of all soft lens fits in the United States (Morgan, 2011).
While these lenses are largely successful due to their physical properties, there have been reports of an association between SiHy lens materials and infiltrates (Kislan, 2010; Szczotka-Flynn, 2007b) or other adverse events (Holden, 2001; Jalbert, 2001; Morgan, 2005b). In the past several years, a type of “sterile” infiltrative keratitis (IK) that is a distinct clinical entity from that previously described in contact lens wearers (Bates, 1989; Baum, 2000; Donshik, 1995) has presented to my practice.
Contact lens-associated infiltrates/infiltrative keratitis (CLAIK) presents as sterile with small, superficial, granular infiltrates and may or may not be accompanied by symptoms. In this article we will discuss three cases of CLAIK in patients using SiHy lenses with a multipurpose solution (MPS).
These three cases were chosen as they were representative of the cases of CLAIK that we observed in 2010. Each patient presented with a slightly different clinical picture and baseline characteristics, including gender, eye involvement, conjunctival injection, and slit lamp findings, that are commonly observed in patients who have CLAIK. Each patient also underwent a somewhat different management strategy, including treatment and post-resolution management.
Case Study 1
An experienced 46-year-old daily lens wearer presented to our office with complaints of burning, red eyes for several weeks. She wore balafilcon A (PureVision, Bausch + Lomb [B+L]) lenses and did not have these symptoms with her prior phemfilcon A (Durasoft 2, Ciba Vision [Ciba]) lenses. She was using Opti-Free Replenish MPS (Alcon) consistently for several years and performed digital rubbing to clean lenses nightly. Before her visit, she stopped lens wear for several days and her symptoms resolved. They promptly returned with resumption of lens wear.
As detailed in Table 1, her visual acuity was 20/25 OD and OS with her best correction. Slit lamp examination showed superficial punctate keratopathy (SPK) OS and infiltrative keratitis OD. Pre-auricular lymph nodes were uninvolved, ruling out epidemic keratoconjunctivitis (EKC).
We made a diagnosis of CLAIK and placed the patient on tobramycin and dexamethasone (Tobradex, Alcon) suspension q.i.d. for one week without lens wear. At follow up, visual acuity was 20/20 in each eye and corneas were clear. We prescribed a hydrogen peroxide system, Clear Care (Ciba), for disinfection, and to date she has remained symptom- and infiltrate-free.
Case Study 2
A 17-year-old lotrafilcon B (O2Optix, Ciba) daily wearer presented for an urgent care visit with complaints of sudden blurred vision OD, but was otherwise symptom-free (Table 1). Visual acuity was 20/25 and slit lamp examination revealed non-staining infiltrates OD. In the left eye, visual acuity was 20/20 and no infiltrates were present. The slit lamp examination was otherwise unremarkable. Upon repeat questioning, the patient denied any symptoms or sleeping in his contact lenses. He claimed good compliance with his care regimen (Opti-Free Replenish), but did not perform digital cleaning of his lenses. Contact lens discontinuation was recommended for two weeks.
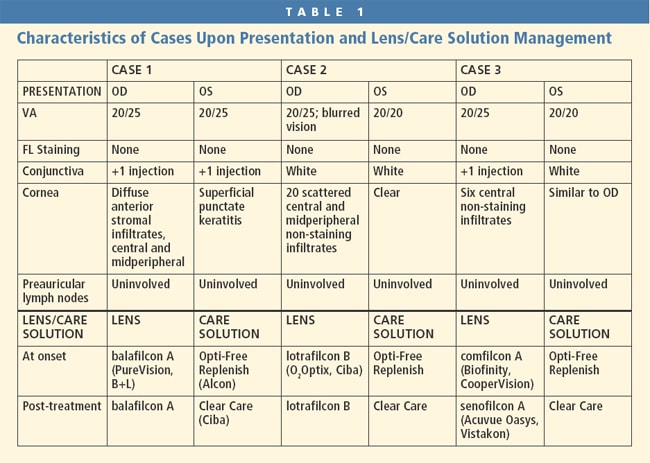
Because the patient was travelling and unable to return for follow up for several weeks, we asked him to resume wear using a new pair of the same lenses but with Clear Care as his new care system only if his vision was clear and he was symptom-free.
At his one-month follow-up visit, visual acuity was 20/20 with his contact lenses, the patient was symptom-free, and no infiltrates were present upon examination. At his annual examination six months later, the patient was free of corneal infiltrates.
Case Study 3
A 16-year-old established patient presented to our office with complaints of burning, tearing eyes that began approximately 24 hours prior to an emergency visit. She described the symptoms as a foreign body sensation.
She was an Opti-Free Replenish and comfilcon A (Biofinity, CooperVision) lens daily wear user (Table 1) and had been successful with this combination for more than a year. She denied extended wear and disposed of her lenses as prescribed to her. Cleaning consisted of rubbing and she rinsed her lenses “about half the time.”
At presentation, visual acuity with eyeglasses was 20/25 OD and 20/20 OS. Slit lamp examination showed non-staining infiltrates OD and OS, conjunctival injection of +1 OD, and no injection OS. No staining with fluorescein (FL) or rose bengal was observed in either eye. She was told to cease contact lens wear and treated with preservative-free artificial tears and loteprednol etabonate (0.5%) drops (Lotemax, B+L) q.i.d. OD and OS.
At the patient's follow-up visit two weeks later, she had no infiltrates and her corneas were clear. She was placed into both new SiHy lenses and a new lens care system (Table 1), and upon follow up was infiltrate- and symptom-free.
Discussion
We have anecdotally noticed an increased occurrence of sterile corneal infiltrates in our practice with SiHy lens wear, and in our experience, it has most often been with the use of Opti-Free Replenish and Acuvue Oasys (Vistakon), though not presented in the cases in this article was the topic of a previous case series (Sacco, 2011). Our observed increase in the number of infiltrative events in users of this care solution with SiHy lenses is in line with those of others (Carnt, 2009; Diec, 2009; Hine, 2008; Kislan, 2010; Reeder, 2011). We have, however, also seen these events to a lesser extent with Opti-Free Express (Alcon), both Renu Fresh and Renu Sensitive (both B+L), private label MPSs, and, rarely, with peroxide systems. These events also seem to be more frequent since mid-2007, at least in our practice. It is entirely possible that earlier cases of what my colleagues and I have termed CLAIK were misdiagnosed as either hypoxic or infectious infiltrative events or even went unnoticed.
While the argument can be made that more cases of CLAIK are being observed with a certain care solution or contact lens due to an increase in market share of those specific products, it is my belief that market share does not explain this increase in full. In agreement with the literature (Stapleton, 2007) during the time period when conventional (yearly replaced) hydrogel lenses were the most widely used, we didn't see as many cases of infiltrates as we have observed with SiHy lenses, possibly due to the total number of lens wearers; and we either did not observe CLAIK or the frequency was low enough that we did not recognize it. When the use of frequent replacement hydrogel lenses became the most widely used lens modality, we may have seen more infiltrates, but I believe not to the extent that we are seeing today. To my knowledge, there appears to be only one study published that describes a similar clinical picture as CLAIK in two patients, and interestingly, these patients were also daily lens wearers who used a Polyquad-based lens care system (Yeung, 1997). So it isn't just because SiHy lenses are used most frequently per se, but that these infiltrative events may be due to some property of SiHy lenses themselves and/or incompatibility with some aspect of a care solution. However, when frequent replacement hydrogel lenses peaked in usage, Opti-Free Replenish was not on the market as it only became available in the last five years. So it is possible that we would have seen more cases of infiltrates and some cases of CLAIK if this care solution were available when conventional and frequent replacement hydrogels were the most commonly prescribed materials. However, this assumes that some property of a specific care solution and SiHy materials is involved in the etiology of these events, which has yet to be proven, but is my belief based on my clinical experience.
Further, based on my clinical experience, I believe that these infiltrative events seem to be unrelated to corneal staining. This is also consistent with recent findings regarding corneal staining and infiltrates as presented in a re-analysis of a prior study (Willcox, 2008) and more rigorous studies (Szczotka-Flynn, 2010) by authors who previously found an association between corneal infiltrates and fluorescein corneal staining (Carnt, 2007a; Szczotka-Flynn, 2007a). I do not believe the cause to be hypoxia, given the very high oxygen transmissibility of SiHy contact lens materials and the daily wear nature most typical of these cases.
Clearly there is room for error and interpretation in the diagnosis of corneal infiltrative events, especially in contact lens-wearing patients. As delineated in Table 2, CLAIK has several distinct characteristics from those typically observed in IK cases. Many, if not most, cases of CLAIK present without the degree of pain and photophobia typical of contact lens-induced peripheral ulcer, IK, microbial keratitis, and contact lens-induced acute red eye (Carnt, 2007a). In cases of CLAIK, all present with multiple epithelial or sub-epithelial infiltrates that are bilateral and central or paracentral in more than 90 percent of instances. In contrast, cases of IK usually have a single, focal infiltrate in more than 50 percent of cases and in all but one study (Bates, 1989) are almost always unilateral (Baum, 2000; Donshik, 1995; Efron, 2005) and located in the peripheral or midperipheral cornea (Bates, 1989; Baum, 2000; and others, full list at www.clspectrum.com/references.asp). Also, there seems to be a grayish, granular type appearance to these infiltrates rather than the globular, focal infiltrates common in infectious or hypoxic etiologies. Similarly, infiltrates in cases of IK appear round, hazy, grayish-white, cloudy, and/or amorphous, which is distinct from that observed in cases of CLAIK. Figures 1 and 2 are representative images of the cases of CLAIK seen in our clinic.
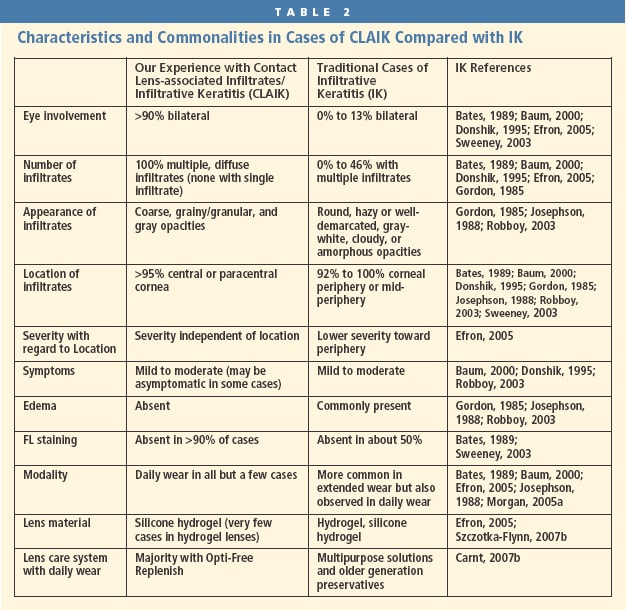

Figure 1. Appearance of infiltrates in a case of CLAIK.
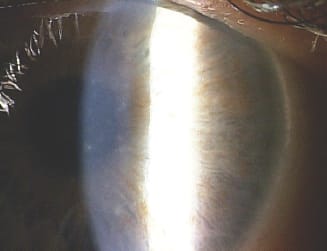
Figure 2. Another view of central infiltrates in the same case of CLAIK.
We likely have much to learn about silicone lens materials and their interactions with the tear film and disinfecting systems. While the physical properties of this material do provide an excellent safety profile, there are reports of increased conjunctival staining (Maldonado-Codina, 2004), mucin ball formation (Tan, 2003), bacterial adhesion (Henriques, 2005), superior epithelial arcuate lesions (SEALs, [Holden, 2001; Jalbert, 2001; Morgan, 2005b]), contact lens-induced papillary conjunctivitis (CLPC, [Dumbleton, 2002; Morgan, 2005b; Skotnitsky, 2005]), and perhaps no change in the rate of microbial keratitis (Stapleton, 2008). While the purpose of this report is not to confirm an association between a multipurpose solution and SiHy lens material combinations with CLAIK, it is further insight, in my view at least, that this association needs further study.
Notwithstanding our findings and experience with SiHy contact lenses in this report, we continue to find more advantages than disadvantages with this class of lenses compared with more traditional materials. For that reason we continue to use this lens material quite readily while paying attention to solution/lens compatibility. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #185.
The author would like to acknowledge BioScience Communications for its support with this article and Tom Kislan, OD, for the use of his photographs.

|
Dr. Sacco is the owner of the Sacco Eye Group in Vestal, N.Y. Dr. Sacco is residency trained in primary care from the Pennsylvania College of Optometry and is active in clinical research, hospital-based physician education. He is the Immediate Past President of the New York State Optometric Association. He is also a consultant/advisor to B+L and has received research funding from B+L and Vistakon. |