


Healthcare Reform
Healthcare Reform and Electronic Health Records
It's time to get ready for the upcoming changes in health care delivery. Are you ready?
By Scot Morris, OD
Not only has healthcare reform been front and center within the consciousness of the American people, it has been a daily discussion item for all political figures, media outlets, and anyone who wants to voice his opinion. It will, undoubtedly, play a large role in the upcoming national elections, as well as in the platforms for every political race that will occur in the United States for many years to come. It is a topic that seems to be discussed daily within most medical practices. It appears to be a topic of conversation everywhere we turn because, simply stated, our healthcare system is broken and has been for quite some time.
Because it is so meaningful to all of us, healthcare reform is a very challenging subject to tackle, both politically and financially. Global economic woes have only contributed to our nation's added awareness of the financial realities and long-term viability of maintaining the various healthcare programs to which we, the people, are accustomed. The costs of health care have skyrocketed for most, if not all, Americans. Meanwhile, most of our delivery systems are incredibly inefficient and, in some cases, are actually compromising the health of their participants.
Lastly, the United States is considerably behind most nations on most of the healthcare pillars. Although these facts aren't always easy to accept, let's take an even closer look.
The Financial Facts In the United States, the average person currently spends $7,410 per capita annually (World Bank, 2009), or a collective $2 trillion a year on health care. Even more concerning is that this is an $800-per-person increase in less than three years (World Bank, 2006). A recent article in Bloomberg Weekly (May 17th, 2011) also reported that many states are budgeting that this number will rise more than $1,000 per person in the next three years. This is just the reimbursements and payouts to the medical industry. When we figure in the actual cost of providing this health care (including the true human resources costs, expenses, time, etc.), we could probably quadruple that number.
Are we being proficient in how we manage these financial resources? Are we truly providing the best care for our patients? Are we managing our businesses efficiently? Can we continue this without paying the consequences? How will our children afford the healthcare system we are leaving them?
Healthcare costs have been rising for several years. Expenditures in the United States on health care surpassed $2 trillion in 2006 (the last major healthcare expense census), almost three times the $714 billion spent in 1990 and more than eight times the $253 billion spent in 1980. Slowing down this growth has become a major policy priority, as the government, employers, and consumers increasingly struggle to keep up with healthcare costs. In 2006, United States healthcare spending was about $7,026 per resident and accounted for 16 percent of the nation's Gross Domestic Product (GDP), which gave the United States the dubious honor of spending more on health care as a percentage of GDP than any other country in the world (World Health Organization [WHO]).
Although Americans benefit from this increasing investment in health care, the recent rapid cost growth, coupled with an overall economic slowdown and rising federal deficit, is placing tremendous pressure on the systems we use to finance health care, including private employer-sponsored health insurance coverage and public insurance programs such as Medicare and Medicaid. Since the year 2000, employer-sponsored health coverage premiums have increased by 87 percent. Employers are increasingly shifting costs to their employees in the form of higher premiums, deductibles, and co-payments or, in many instances, eliminating healthcare coverage. With workers' wages growing at a much slower pace than healthcare costs, many face difficulty in affording this growth in out-of-pocket spending. Largely due to the implementation of the Medicare Part D benefit in January 2006, Medicare program spending increased 18.7 percent in 2006. Conversely, because drug coverage for dual eligibles were transferred from Medicaid to Medicare, spending in the Medicaid program decreased 0.9 percent, the first decrease in Medicaid spending since its creation in 1965. However, it still accounts for 40 percent of national health spending and comprises one of the largest items in state budgets.
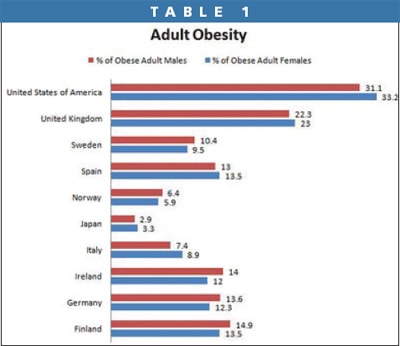
The Numbers To put the state of our healthcare system in perspective from the world economy level, here are some statistics comprised by WHO. The United States ranks 37th in the world in healthcare performance, just behind Costa Rica and just ahead of Slovenia. We rank 72nd in world healthcare rankings out of 122 countries. We rank 24th in life expectancy. We spend 20 times more than our neighbor Cuba does and have approximately the same life expectancy (UC Atlas of Global Inequality). We rank first in obesity (Table 1) and healthcare costs per capita. In fact we spend almost as much per capita as the next three countries combined and more than the bottom 22 combined.
Remember that our current administration, the government, and the insurance companies are not the enemy. The way in which we have conducted health care has evolved, and it has to evolve to survive. The way in which we have practiced medicine in this country has not been successful when you look at the details.
Solutions to our Healthcare System
Undoubtedly, solving our healthcare issue will be no easy task and will take decades to get spending and access issues under control. However, other issues pose even larger problems because they cross the line between the private and public sectors, as well as adversely impact the very fabric of how healthcare has been implemented for decades. There are five basic pillars to healthcare reform that we need to discuss.
1. Insurance Companies and the Business of Health Care With company dividends reaching into the hundreds of millions for the upper echelon of the various private healthcare companies while the provider reimbursements are being decreased and overall consumer benefits are being reduced from every angle, you have to wonder, “Where is all the money going?” Here is where we have to separate private insurance from public entitlement plans such as Medicare and Medicaid.
Third-party insurance is capitalism at its finest; it is about providing a service, but ultimately it is still about the bottom line. Business is business, even if it is at the expense of an individual's personal longevity. Anyone who buys third-party insurance is accepting of the benefits of that business venture just as if they were buying property or signing any other kind of business deal. The risks may be greater because there is no “standard” for human life.
Contrast this with public healthcare programs that are essentially government-sponsored socialized medicine that has no capitation or utilization restrictions. It is then important to consider that Medicare was never devised for the utilization of expensive technologies; life-sparing, astronomically expensive surgeries; or to take care of the general population who live into their 80s. At the time that Medicare was created, technology consisted of X-rays and a stethoscope, and the life expectancy was about 62.
Private health care and public health care have little-to-nothing to do with one another, but we the people don't always visualize it that way. This is at the root of the insurance dart board. Whether this country moves toward increased taxes and a more socialized medicine model like most of the world or whether the United States once again sets a new world standard and completely privatizes health insurance for all people is yet to be determined. What is apparent, however, is that health insurance as we know it is going to change dramatically in the next few years.
2. Testing, Tort, and Turning the Tide Related to health insurance is the provider side of the discussion. Physicians in the United States provide more diagnostic testing and more expensive testing compared to any other healthcare system in the world. Most physicians will never freely admit that they perform unnecessary tests or duplicate tests with acceptable reliability variables to increase personal reimbursement, prevent potential litigations or wrongful practices suits, or both. However, this practice is pervasive in the American medical culture. This has led to exceptionally high utilization of diagnostic tests such as magnetic resonance imaging (MRI), carotid doppler, and even many ocular diagnostic tests when simple observation and some clinical experience could many times lead to the same ultimate results. Secondly, costs for diagnostic tests here are substantially higher compared to the rest of the world. For example, the fee assessed for an MRI performed in the United States is in the $2,000 range, whereas in most of Europe it is about $50.
At the root of this mentality is tort reform. To truly change the mindset of many physicians, we need to change the tort laws to protect physicians as well as healthcare consumers. Congress has visited and revisited the ideas of tort reform as it applies to health insurance malpractice claims. So far, not much has resulted from those discussions to limit the litigation-happy population and the associated lawyers from filing suit for wrongful practice issues against anyone they see fit. It may take generations of physicians to eliminate the fear instilled upon most physicians over the last few decades as it relates to excessive testing.
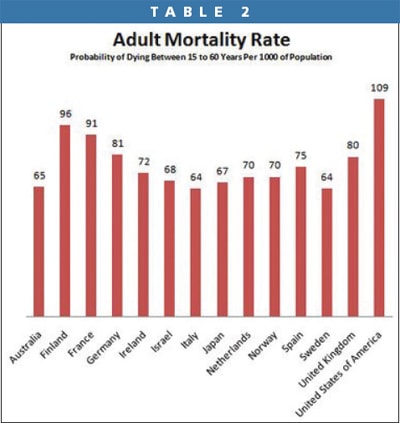
3. Food, Pharma, and the American Way There are so many variables to the actual etiology behind the growing levels of obesity in our country, but many people point to large food companies as one of the biggest culprits in America's healthcare issues and may play an important role in a higher than average adult mortality rate (Table 2). It is easier and less expensive to purchase a “Happy Meal” than a salad. It is less expensive to purchase a sugar-loaded, caffeine-spiked energy drink than it is to buy a bottle of water of the same volume. We could devote book chapters to the food conspiracy theories, but one factor is certain: Americans love to eat and then look for the quick fix to counteract all the physiological negatives that are associated with our often less-than-optimum dietary habits. Drug companies are ever-so-happy to indulge our overindulgence by creating drugs for the array of healthcare issues that our diet has created. According to “Expenditures for the Top Five Therapeutic Classes of Outpatient Prescription Drugs, Medicare Beneficiaries, Age 65 and Older,” the top five drug classes that treat hypertension, hypercholesterolemia, hyperglycemia, anxiety, depression, and gastric reflux disease account for 66.2 percent of all drug-related healthcare expenditures in that age group, with 22.7 percent being for metabolic altering agents such as antihyperlipidemic and antidiabetic agents alone. Of course many critics claim that pharma companies have helped create the need for their drugs by influencing studies to lower certain treatment criteria or creating certain drug classes to treat conditions that some simple exercise and a little time outdoors would probably alleviate. In essence, pharma companies are helping to promote the American mindset of “there is a drug for that”—so why worry about fixing the actual problem? This brings us to the next big issue.
4. Personal Responsibility Many critics of healthcare reform have commented that ultimately, the primary issue with our healthcare system is personal responsibility or, more correctly, the “lack of” personal responsibility. We now live in an entitlement society in which it is always someone else's fault or someone else's responsibility, but ultimately “we” are different and deserve something and anything we want. This mindset can be extended to our society's personal health and lifestyle choices, litigation issues, food consumption, and countless other discussions. There are no easy solutions, and many sociologists estimate that it may take generations to change our societal views and personal habits. In the past decade we have seen the green movement, the energy movement, and we are currently in what many call the “return to thrift” movement. Steps need to be taken. One of the most promising steps toward healthcare reform has actually been the movement toward evidence-based medicine.
5. Evidence-Based Medicine Some term this “value-based medicine” and others term it “evidence-based medicine” (EBM), but the basic tenet is a system based on payment for performance by the healthcare providers and coverage values for the healthcare consumers that are based on certain health and lifestyle risk criteria. The movement toward EBM has been in process for almost 15 years, although it is just beginning to be a common discussion topic in the medical community and the general population. At the root of EBM is the ability for all physicians around the country to talk the same language and use a universal health delivery system.
EBM and the Healthcare Reform Process
One of the major foundations of healthcare reform and, more specifically, EBM is adoption and utilization of electronic health records (EHRs). This process began in 1996 with the Health Insurance Portability and Accountability Act (HIPAA). It was followed by the Physician Quality Reporting Initiative (PQRI) and continues with the enhanced vocabulary of the pending International Classification of Diseases (ICD) update to ICD-10, and finally, the universal language of EHRs. The ultimate goal is to develop an evidence-based medicine component of EHRs. These capabilities are expected to drive the “improvement in care” aspect of EHRs by guiding us to community- or profession-based clinical recommendations during documentation and case management.
There are currently no well-documented rules on exactly what EBM will consist of, but there is a basic blueprint in progress that has been present for more than two decades, although it has been a slow, tedious, and somewhat challenging process. Changing not only the entire fragmented healthcare system but also how consumers utilize and perceive healthcare is a daunting task. It will take the proverbial baby steps to change the entire process. To more fully understand the process, it is important to review the key components to EBM.
The first step in the process of changing the American healthcare system is to protect and provide security of this valuable personal health information. This concept resulted in the Health Information Portability and Accountability Act of 1996, more commonly known as HIPAA. Through the development of these protocol rules, the mission was to provide some scrutiny of a healthcare consumer's personal health information.
1. PQRI Following good business strategy and scientific method, the next step would be to undertake a small quality assessment sampling to verify whether a specified set of conditions could be monitored, tracked, and modified. The 2006 Tax Relief and Health Care Act required the establishment of the PQRI. The program name was changed to Physician Quality Reporting System (Physician Quality Reporting) in 2011. PQRI was also a sampling to see what the attendance rate, if you will, would be for the generalized healthcare community. By providing a small reimbursement entitlement to those providers who participated within this sampling method, the hope was to gain momentum and information by enticing a certain group of providers to participate. The ultimate goal is to establish certain criteria and protocols for the validation of the EBM outcomes.
2. E-Prescribing The next step was to begin the process of controlling expenses, tracking drug utilization, and designing the initial framework for a national healthcare database. The national pharmacy database has accomplished exactly that. The Drug Enforcement Agency's (DEA) Electronic Prescriptions for Controlled Substances rule effective June 1, 2010 allowed credentialed and authorized providers to voluntarily electronically sign and forward prescriptions to pharmacies. E-prescribing is also one of the 20 criteria outlined as part of the incentive payment criteria. The ultimate goal is to save dollars and lives by preventing costly cross-reactions, side effects, and over-utilization of certain drugs without just cause.
3. ICD-10s As with any language, the larger the vocabulary, the more information that can be attained, observed, and analyzed. Essentially expanding to the world standard on ICD is the next viable step in the process toward EBM. The changeover from the old ICD-9 system to the ICD-10 system will occur Oct. 1, 2013, although healthcare providers will be required to have such software installed in their office systems by Jan. 1, 2012. Moving from the 19,000 code ICD-9 database to the world standard ICD-10 database that utilizes more than 68,000 codes will increase the specificity of various disease states as well as related comorbidities. This will allow for more accurate diagnosis and treatment monitoring. ICD-10s will also expand healthcare providers' vocabulary by increasing the specificity of disease states involved. This coding system is required for all public and private health sector plans. This conversion will apply to all claims, not just electronic ones. Tools are already in development to allow conversion of ICD-9 codes to ICD-10s. You can find more information on these tools at www.cms.gov/ICD10.
4. Electronic Health Records Lastly, once the other criteria have been satisfied, all providers and users of healthcare information need to be able to share information or have a universal language. By developing a nationalized standard, currently termed Certification Commission for Healthcare Information Technology (CCHIT), not only can our healthcare system have dramatic increases in healthcare information portability but also save millions, if not billions, of dollars annually on unnecessary tests, visits, and procedures, which will hopefully ultimately save tens of thousands of lives. The National Health Information Network will be formally introduced in 2014 to establish standards for health information exchange.
To encourage adoption and utilization of EHRs, Congress set aside $19.2 billion as part of the American Recovery and Reinvestment Act (ARRA) to encourage doctors and hospitals to move quickly to adopt “qualified and meaningful use” systems. According to the Health Information Technology for Economic and Clinical Health (HITECH) provision of the stimulus plan, certified EHRs must allow for the following:
• Electronic prescribing (e-prescribing)
• Exchange of information to enable improved health care (portability)
• Reporting of clinical quality information
Under the “meaningful use” criteria, practitioners who satisfy the implementation requirements are eligible for bonus payments starting in 2011. At this time, these incentives are related only to a provider's Medicare reimbursement. Commercial payers have not publicly indicated their plans to follow suit. Medicaid panelists may also be eligible for additional sums not to exceed $63,750, depending on individual state mandates.
Keep in mind that more than 70 percent of the total incentive money will be disbursed within the first two years. Providers engaged in PQRI and electronic prescribing can earn an additional $6,000 to $8,000 per year beginning immediately. Healthcare professionals who do not adopt EHRs by 2015 will be penalized by a 1 percent to 2 percent reduction in Medicare reimbursement rates.
Treatment Options and EHRs' Role in EBM
EHRs will allow for a far greater sampling than what the PQRI initiative accomplishes. Unlike traditional retrospective and prospective drug or disease condition studies, a very large sampling size will ultimately be achieved. Analyzing this data will allow comparison of certain risk factors, diagnostic devices, and various effective treatment protocols to be developed. Whether it is the analysis of drug effectiveness or potential risk issues, we may be able to have greater information on certain drugs or the success rate of certain procedures across the general population. This will provide much more “real life” information compared to the current process that involves interpolation of test results in the study population to the target population or an educated guess on the potential risks or complications that could exist. EBM would essentially also eliminate or penalize providers who order unnecessary tests and are prescribing ineffective treatments. This will ultimately require a dramatic change in payment or reimbursement structure and is likely decades away.
EHRs' Role in EBM EHRs are really the backbone of the EBM movement. Without EHR, there would be hundreds of people talking and no one able to understand what the other is saying—the proverbial EHR “Babel” that we currently accept as truth today. The goal of EBM affects not only EHRs, but also communication and management issues.
EHRs should contain an integration of clinical decision support and best practices, support e-prescribing, and have the capability to track and analyze outcomes.
Communications Software The communication software associated with the EHR must be able to securely transfer protected health information (PHI), according to the HIPAA criteria and connect to all areas of health care.
Management Capabilities Lastly, EHRs will allow for enhanced business management and streamlining of the healthcare system. This ultimately is what will save some of the programs that are currently at risk.
Another part of healthcare reform that was signed into law on March 23, 2010 was the Patient Protection and Affordable Care Act. This law had several positive ramifications for our profession including prohibition against discrimination against groups of providers, children's vision care as an essential health benefit, and the creation of state-based health insurance exchanges in which consumers can shop for and purchase healthcare insurance.
Your Role in EBM and Our Healthcare System
The final outcome of these processes will undoubtedly have a significant impact on eye care. There will be changes in reimbursement, coverage, access to providers, and, most importantly, how medicine operates. A crucial cornerstone to the pending health care changes is utilization of technology, more specifically EHR. There is one certainty; eyecare practitioners cannot stop the coming changes. As a profession, we need to be very cognizant of these changes and how they will affect our profession and practices and embrace the process in a proactive manner. What can you do now in preparation?
Step 1 Select, install, integrate, and implement EHR—soon.
Step 2 Engage in PQRI.
Step 3 Initiate e-prescribing.
Step 4 Become a “meaningful” user of an HIT. To become more familiar with the various components of the incentive programs, visit www.cms.gov/EHRIncentivePrograms.
Need another reason? Fortunately, EHR software solutions are advancing rapidly. Early adopters are already benefiting from integrated diagnostic technology and business operational technology such as document management, inventory management, and accounts receivable automation.
More impressive is the rapid advancement of clinical decision support (CDS) in some of the current EHR programs. This tool helps clinicians determine better standards of care, establish new practice guidelines, and deliver overall better care by providing true outcomes-based reporting intelligence. CDS also allows for more accurate management of inventory, human resource workflow, marketing intelligence, and benchmarking.
Summary
With the push for value-driven health care and, eventually, EBM, CDS features will be instrumental in achieving better clinical outcomes, higher payment for performance, and increased operational efficiencies in every aspect of the eyecare practice of tomorrow. Will you be on board? CLS
For references, please visit www.clspectrum.com/references.asp and click on document #189.

|
Dr. Morris is medical director, Eye Consultants of Colorado, LLC, and CEO of Ocular Technology Solutions, Inc. He is a consultant to Alcon, Allergan, AMO, Marco, Luxottica, Inspire, GPN, and Com-Squared. He can be reached at scot@ots-consultants.com. |