


Contact Lens Case Reports
Anatomical Challenges of the Aging Eye

By Patrick J. Caroline, FAAO, & Mark P. André, FAAO
This 54-year-old presbyope was interested in multifocal contact lenses. His spectacle Rx was +1.50D −1.25D x 178 OD and +1.50D −1.25D x 004 OS with a +2.50 add OU. Everything looked fairly straightforward for multifocal GP lenses, and the patient was diagnostically fitted with anterior aspheric lenses. At the 1-week follow-up visit, he had adapted well to the lenses and had only minor visual complaints at distance; however, he had significant concerns about his 20/50 near acuity. As we have done hundreds of time before, we increased the minus asphericity on the anterior surface of the lens to increase the effective add power. With the new lenses, the patient experienced ghosting at distance with little improvement in his near vision.
Why do some patients fail to achieve adequate distance and near optics through their multifocal soft and/or GP lenses? The problem often lies not in the design of the lenses but with the aging eye itself.
Aging Optical System
More than a simple loss of accommodation, presbyopia carries with it an aging optical system that creates significant challenges for all contact lens modalities. Perhaps the greatest anatomical challenge is senile miosis, which is an age-related decrease in pupil size. With simultaneous-vision lens designs, the only optics available to the patient will be those present over the pupil. Therefore, in a 54-year-old presbyope, distance, intermediate and near optics must be contained within the center 3.5mm of the contact lens. That is a lot of optics for a very small area of real estate. As shown in Figure 1, the ultimate visual performance of center-distance or center-near lens designs will be dominated by pupil size. The smaller the pupil, the less the opportunity to achieve the desired 50/50 distribution of light (50 percent for distance viewing and 50 percent for near).
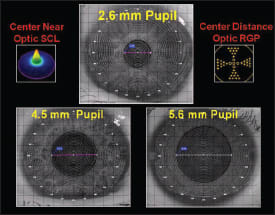
Figure 1. Pupil diameter dramatically affects the optics of center-near and center-distance lens designs. The smaller the pupil, the more compromised the optics.
With aspheric optics, centration is paramount to optimum optical performance. Any decentration, i.e., "translation," will induce significant higher-order aberration, including radial astigmatism, coma and spherical aberration. Therefore, it is not surprising that with multifocal contact lenses, the number of optical aberrations induced over an already compromised (aging) visual system are simply too great for many patients to overcome.
Today, we teach our students that aspheric, center-distance GP and center-near soft lens designs provide a reasonable, binocular (non-monovision) option for many patients with emerging and early presbyopia. However, the optical success of GP and soft multifocal contact lenses will often be predicated on a number of anatomical features that include pupil diameter, anterior chamber depth and corneal radius of curvature.
Meeting Anatomical Challenges
Our patient was ultimately fitted with translating GP lenses and today, he enjoys his clear, binocular distance and near vision. The moral to this story is simple: because of the anatomical, physiological and optical demands of the aging eye, the non-pupil dependent optics of translating lens designs are tough to beat. CLS
Patrick Caroline is an associate professor of optometry at Pacific University. He is also a consultant to Paragon Vision Sciences. Mark André is an associate professor of optometry at Pacific University. He is also a consultant to CooperVision.