


DIAGNOSTIC TECHNOLOGY
Advanced Technology in Contact Lens Practice
Key technologies incorporated into contact lens practice can help improve specialty lens fitting success rates.
By Robert Davis, OD, FAAO, & S. Barry Eiden, OD, FAAO
In our practices, the days of refraction, Ks, and diagnostic lenses seems like a distant memory. Our incorporation of advanced diagnostic technologies has allowed us to individualize our contact lens management strategies, resulting in optimized outcomes. We are able to screen our patients to pre-determine whether there is an increased risk for contact lens-associated dry eye, visual irregularities that could limit the quality of optical performance, and corneal geometries that could result in unstable physical fits. We can also differentially diagnose visual difficulties that standard methods cannot detect. The use of these technologies further allows us to customize our selection of materials, optical designs, and lens shape parameters, which will result in the highest quality vision, comfort, and physiological response.
The use of advanced technologies in contact lens practice further differentiates contact lens specialists from other eyecare practitioners who also fit contact lenses. These technologies can positively influence patient perception, building confidence and going far in fostering referrals.
We will review a number of key technologies that we utilize on a daily basis that have had the greatest impact on the ongoing success of our contact lens specialty practices.
Corneal Tomography
Corneal topography has been a highly useful technology in contact lens practice over the past 20 years. Topography can increase your diagnostic capabilities. However, anterior corneal Placido-based topography provides only a limited look at the corneal geometry.
Pentacam corneal tomography (Oculus Corporation, Wetzlar, Germany) provides a more extensive look at the cornea. Utilizing 360-degree Scheimpflug imaging (Figure 1), the Pentacam provides true elevation data of both the anterior and posterior corneal surface, then calculates a three-dimensional model of the anterior eye segment based on the measured elevation data. True anterior corneal elevation data allows us to accurately predict the lens-to-cornea fitting relationship, especially in cases of corneal irregularities.
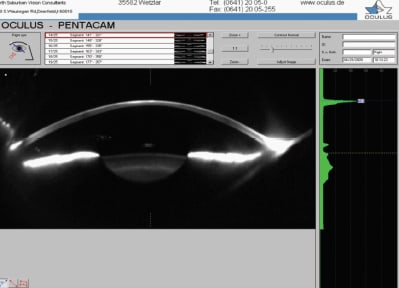
Figure 1. Pentacam Scheimpflug image.
Most importantly, Pentacam provides an analysis of the posterior corneal surface. This is invaluable when evaluating patients who have ectasia such as keratoconus (Figure 2), pellucid marginal degeneration, or surgically induced ectasia. By evaluating both the anterior and posterior segments of the corneal surface, it becomes quite evident when we are dealing with contact lens-induced corneal distortion versus true ectatic disease. The ability to monitor progression of corneal ectasia with Pentacam is incomparably superior to traditional forms of topography.
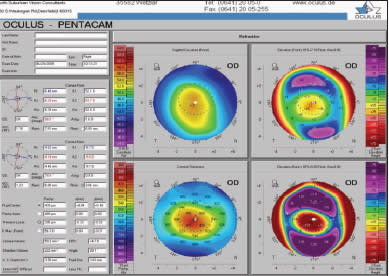
Figure 2. Pentacam refractive “quad” map: keratoconus.
Additionally, Pentacam optically measures corneal thickness throughout the entire surface, thus providing much more extensive pachymetric data when compared to results from ultrasonic pachymetry. Evaluation of pachymetric progression from thinnest point out to thickest point is also highly diagnostic of corneal ectasia. Pachymetry measurements are also extremely useful in diagnosing and monitoring corneal edema, whether due to disease or contact lens-induced hypoxia.
In addition, the Pentacam has other features that provide expanded diagnostic capabilities such as the ability to measure densitometry values of media opacities, to provide an analysis of corneal aberrometry, and to apply contact lens fitting designs through the Oculus Pentacam contact lens fitting software and simulated fluorescein patterns.
We use Pentacam corneal tomography on all contact lens patients at least annually, on all patients who have undergone corneal surgical procedures (such as penetrating keratoplasty, Descemet's stripping endothelial keratoplasty, etc.), on all patients who have ectatic disease, and on all patients who have undergone refractive corneal surgery. The diagnostic applications of Pentacam go far beyond those mentioned in this article and make the instrument one of the most versatile and important of our advanced diagnostic technologies.
Applicable CPT codes:
● Corneal topography – 92499
● External ocular imaging – 92285
● Optical pachymetry – 92499 (Cannot use 76514 because it refers specifically to ultrasonic pachymetry)
Specular Microscopy of the Corneal Endothelium
The corneal endothelium is a single layer of cells that maintain the thickness and clarity of the cornea. By continually “pumping” water out of the stroma into the anterior chamber, the endothelium offsets the natural tendency of the cornea to imbibe water. Without proper functioning of the endothelium, the cornea thickens significantly and eventually loses its transparency. Such is the case in significant endothelial disease such as Fuchs' dystrophy.
A key—yet often overlooked—form of endothelial disease is associated with long-term contact lens wear, especially when associated with subsequent chronic hypoxia. Contact lens-induced endotheliopathy (Figure 3) is a potentially serious condition that needs to be identified and addressed in its early phases to avoid long-term clinical implications. Contact lens-induced endotheliopathy is also a diagnostic entity that identifies visual compromise in problematic contact lens patients.
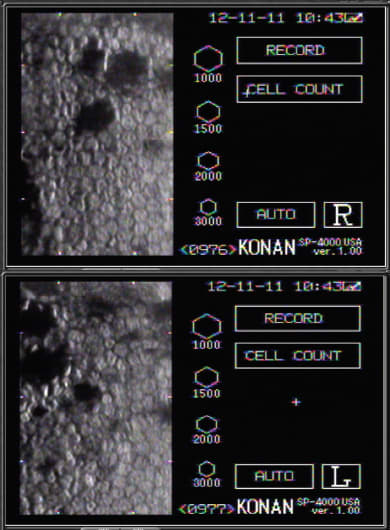
Figure 3. Contact lens-induced endotheliopathy.
In recent years clinically applicable forms of specular microscopy have allowed clinicians to identify corneal endotheliopathy associated with corneal diseases, contact lens wear, trauma, inflammatory eye diseases, and other conditions. Specular microscopy is a simple-to-perform and non-invasive procedure that provides invaluable information on endothelial cell density, cell size variations, and cell shape variation as well as central corneal thickness measures. Abnormality in corneal cell size variability is referred to as polymegethism. Abnormality in the normally hexagonal cell shape is referred to as pleomorphism. Finally, cell density can be reduced beyond normal age-related decreases in the presence of conditions that result in endotheliopathy.
We use a Konan specular microscopy system (Konan Medical, Figure 4) in our practices as a screening procedure for all contact lens patients as well as for other patients who might be at risk for endothelial disease (such as patients who have diabetes, glaucoma, history of ocular inflammation, or prior ocular surgery). If a non-quantified screening suggests the presence of endotheliopathy, then we perform a fullquantified analysis. Screening procedures are not reimbursable from third party payers; however, full-quantified specular microscopy is a reimbursable procedure if accompanied by acceptable ICD diagnostic codes. In our practices, we incorporate endothelial health screening as part of either a general ocular health screening or contact lens diagnostic evaluation.

Figure 4. Konan Specular Microscopy System.
Applicable CPT code: 92286
Accepted ICD codes for CPT 92286:
● 371.57 (endothelial dystrophy)
● 371.20-371.24 (corneal edema)
● 371.58 (posterior polymorphous corneal dystrophy)
● 371.57 or 364.51 (irido-corneal-endothelial syndrome)
Non-Invasive Tear Film Analysis
The ability to quantitatively analyze tear film status without physically influencing the ocular surface provides an accurate and valid means to assess patients for potential dry eye disease. You can perform a non-invasive assessment of tear meniscus height using new software provided with the Oculus Keratograph Topography System (Oculus Corporation, Wetzlar, Germany). Tear meniscus height is an indicator of ocular surface tear volume. Other more invasive and less direct indicators of tear volume include the Schirmer test and the Phenol red thread test.
The Oculus Keratograph measures the inferior tear meniscus height via imaging of the anterior ocular surface and projection of a small horizontal light that reflects off of the top of the tear meniscus. The instrument's software creates a caliper with which you can directly measure the height of the inferior tear meniscus in millimeters (Figure 5).

Figure 5. Non-invasive tear meniscus height measurement with Oculus Keratograph.
Non-invasive tear breakup time has been previously performed by observing keratometry mires: practitioners would ask patients to hold their lids open and then note how much time passed before the mires became irregular. However, when utilizing the Oculus Keratograph software for non-invasive keratometric tear film breakup time (NIKTBUT), the computer analyzes the reflected Placido ring mires and accurately measures the breakup time throughout the surface measured. Detailed time measures of localized tear breakup are recorded to the 0.10 of a second. Breakup times of greater than 14 seconds are considered normal, those between 13 and 8 seconds are considered borderline, and those that are 7 seconds and below are considered abnormal. A cluster of at least four points with reduced NIKTBUT is considered clinically significant. The system allows you to show a video representation of the measurement in real time in which red spots form over the corneal image as the tear film breaks up at that location (Figure 6).
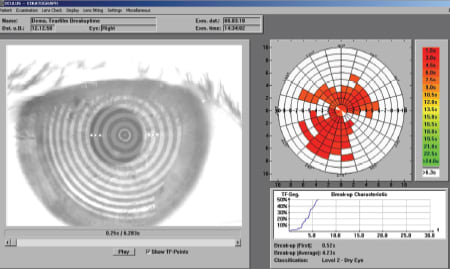
Figure 6. Non-invasive keratometric tear breakup with Oculus Keratograph.
We perform non-invasive tear analysis as part of our baseline contact lens diagnostic evaluation as well as for symptomatic and clinically significant dry eye disease cases. Along with other diagnostic tests and subjective dry eye history, it allows us to more accurately diagnose dry eye disease as well as to pre-determine which patients may be at higher risk to experience contact lens-induced dry eye.
Applicable CPT code:
External ocular imaging – 92285
Tear Osmolarity
Patients experiencing dry eye symptoms present commonly in eyecare practice. According to the Dry Eye Work Shop (DEWS), the prevalence of dry eye ranges between 5 percent to 30 percent among patients age 50 years and older. The authors of the report define dry eye as “a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbance, and tear film instability with potential damage to the ocular surface. It is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface.”
Tear osmolarity is a biomarker that can assess the presence and degree of dry eye and can be used to measure improvements that result from a prescribed therapy. Elevated tear osmolarity has high positive predictive value for the presence of dry eye. Dry eye disease affects osmolarity homeostasis, responding to internal or external stress from systemic disease, hormonal change, post-surgical recovery, blepharitis, and contact lens wear.
Tear osmolarity can be measured using a hand-held instrument called the TearLab Osmolarity System (TearLab Corporation) that obtains a 50nl sample from the inferior tear lake near the lateral canthus. Collection of the specimen is user-friendly and fast without disturbing the tear film. This specimen is directed onto a disposable chip that performs the analysis, and a separate desktop machine quickly generates a read-out. An osmolarity reading of greater than 305 may indicate dry eye disease. Not only does osmolarity increase with more advanced dry eye disease, but asymmetry of findings between the two eyes is also greater with more advanced disease (Figure 7).
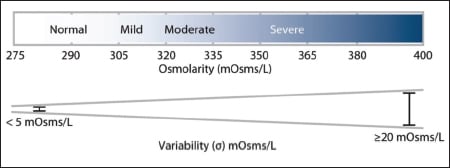
Figure 7. Relationship between dry eye severity and tear osmolarity and variability.
We perform tear osmolarity measurements for all patients undergoing an initial contact lens fitting or refitting procedure. Routinely measuring tear osmolarity for our contact lens patients enables us to select the most appropriate contact lens material, replacement frequency, and care system. We also take a baseline osmolarity measurement for every patient that is referred for cataract or refractive surgery. The data aids in preparing patients for possible post-surgical complications and can serve as an indication for prophylactic therapies for an improved outcome.
Tear osmolarity also provides additional data for the frame selection for dry eye patients. With the osmolarity data, we can select a frame that will protect the corneal surface and minimize evaporation. Additionally, patients who are currently taking topical ocular medications—such as our glaucoma patients—often have elevated tear osmolarity. Selecting medications that have more “cornea-friendly” preservatives or selecting unpreserved therapies improves our patient's compliance by reducing discomfort caused by a compromised ocular surface.
Applicable CPT Code:
● Microfluidic analysis utilizing an integrated collection and analysis device – 83861 (effective January 1, 2011). This is a unilateral test with the second eye submitted using a “59” modifier.
Aberrometry
Traditional clinical refraction aims at correcting spherical and astigmatic ametropia, which are considered low-order optical aberrations. Our vision can be negatively impacted by many other vision anomalies that are termed high-order optical aberrations (HOAs). These HOAs, such as spherical aberration, coma, trefoil, quadrafoil, etc., can cause subjective visual symptoms that cannot be addressed simply by the refractive correction of low-order aberrations.
All forms of optical aberrations (high- and low-order) can now be clinically measured by instruments called aberrometers. Not only can these instruments measure all forms of aberrations, many can also identify the source of the aberrations by separating internal versus external (corneal) aberrations.
Today's aberrometers are typically multifunctional. For example, the Discovery Aberrometer (WF Devices, Figure 8) that we utilize functions as an auto-refractor, auto-keratometer, topographer, pupillometer, and aberrometer. Certain clinical entities such as keratoconus, cataract, dry eye/ocular surface disease, and post-refractive surgical cases are examples in which HOAs can cause symptoms that are not properly addressed by traditional refractive correction (Figure 9). In the past, performing aberrometry was not only impractical clinically, but the outcomes only identified the presence of clinically significant HOAs. There was little we could do to address these problems.
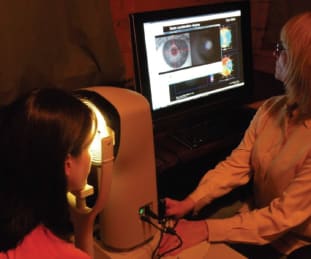
Figure 8. Discovery Aberrometer.
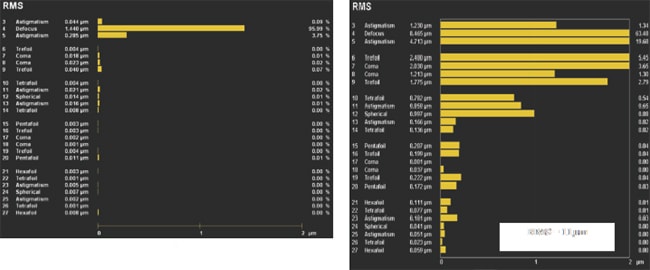
Figure 9. Aberration graph showing only low-order aberrations (left), versus an aberration graph showing both low- and high-order aberrations in keratoconus (right).
Today, however, we are starting to be able to correct HOAs. Wavefront refractive laser treatments, individualized spectacle lens corrections that incorporate HOA control, and HOA-control contact lens designs (both population-based and customized) are being developed and are showing great promise for correcting HOAs. HOA correction can assist with management of visual distortions associated with various eye diseases and also may improve vision function for normal eyes, thus providing “high definition vision.”
Contact Lens Verification
Practitioners take for granted that the power of a contact lens is exactly the same as the power indicated on the contact lens label. You may also assume that the lens power is accurate across the entire optic zone. Measuring a contact lens with a lensometer is a crude method of verification, especially with soft lenses—both the hydration and placement on the lensometer must be accurate.
The Nimo contact lens power and wavefront measurement device by Lambda Technologies (Nivelles, Belgium) provides accurate power distribution maps across the surface of a contact lens and other optical devices (refractive intraocular lenses, diffractive intraocular lenses, and spectacle lenses). Understanding the optics of a contact lens design will help with appropriate lens selection and will improve our ability to problem solve our most difficult patients.
The Nimo power gradient describes the optics of a contact lens in a map configuration that expresses how an image focuses on the retina. With this knowledge, lens selection becomes more simplified and accurate. We can eliminate lens designs that do not perform optimally on a patient's eye. Nimo technology provides practitioners, manufacturers, universities, and research centers with a readily available, open framework technology to determine the power profiles and wavefront characteristics of contact lenses of all designs (spherical, aspheric, toric, and multifocal).
Anterior Segment OCT
Our understanding of a lens on the surface of the eye is uniquely enhanced by anterior segment optical coherence tomography (OCT) imaging. OCT devices have been used to study many aspects of the ocular anterior segment including the whole cornea; the epithelium; anterior chamber width, depth and angle; the flap after laser-assisted in situ keratomileusis (LASIK); corneal foreign bodies; and the tear film.
An OCT resolution of 5mm and faster speed of A-scan (26,000 scan/sec) is available with the 840nm spectral-domain (SD) OCT RTVue-100 (Optovue, Inc.). Higher resolution SD-OCT may be better than time-do-main OCT for detecting keratoconus based on the distribution of corneal thickness. The OCT instrument measures global pachymetry to demonstrate the exact position and amount of corneal thinness at the apex of the cone. Anterior segment OCT findings have been used to specify peripheral fitting characteristics of scleral lenses based on anterior segment OCT measurements taken with the Visante OCT (Carl Zeiss Meditec). These instruments provide an image of the cornea and sclera out to a chord diameter of 14mm to 16mm that could be useful for individual patient baseline measurements. The information obtained from OCT imaging may eventually change the way we design contact lenses. Visualizing the fitting characteristics of a contact lens on the cornea precisely quantifies the lens-to-cornea fitting relationship.
In addition, OCT studies (Wang et al, 2006; University of Rochester Eye Institute, 2010) demonstrate why artificial tears or medications provide a therapeutic effect. OCT imagery can pinpoint ripples or breaks in the tear film that prevent the tears from moistening the corneal surface. We can document how long artificial tear drops stay on the surface of the eye. This allows us to adjust the frequency of drop instillation. OCT images can also identify scar formations and the depth of the corneal damage, aiding in the therapeutic approach.
Applicable CPT code: 92132
Conclusion
The application of advanced diagnostic technologies in our practices has improved our ability to provide our patients with optimal visual outcomes, lens comfort, and physiological response. In addition, these technologies have resulted in higher contact lens success rates, fewer patient dropouts, and increased practice efficiency. Incorporating advanced technologies into your practice can help you distinguish yourself as a true contact lens specialist. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #183.

| Dr. Davis is co-founder of Eye-Vis Eye and Vision Research Institute. He practices in a suburb outside Chicago. He is an advisor or consultant to CooperVision and SynergEyes, has received research funds from Cooper-Vision and B+L, and has a proprietary interest in SpecialEyes and Alternative Vision Solutions |

| Dr. Eiden, co-founder of Eye-Vis Eye and Vision Research Institute, is president of a private group practice in Illinois. He has a financial interest in Alternative Vision Solutions, LLC, is a consultant or advisor to Ciba Vision, CooperVision, SynergEyes, Alcon, and SpecialEyes, and has received research funds from Vistakon, CooperVision, and B+L. |