


Research Review
Should You Use Corticosteroids to Treat Bacterial Keratitis?

By Loretta B. Szczotka-Flynn, OD, PHD, MS, FAAO
Population-based incidence data estimates that 30,000 Americans and 500,000 persons globally experience microbial keratitis (MK) each year (Wilhelmus, 2002). Although the microorganisms responsible for the infection can usually be effectively treated with antimicrobial therapy, sight-limiting corneal scarring often leaves the patient with visual loss after the infectious process has resolved. Globally, more than one million people are visually disabled in one eye because of microbial corneal infection (Wilhelmus, 2002).
Fortunately, in contact lens wearers the rate of visual loss after MK is relatively low. Stapleton (2008) estimates that 13.9 percent of contact lens wearers experience visual loss after an episode of MK.
Nonetheless, MK continues to plague contact lens wearers and the practitioners who treat them. Despite our best efforts to improve contact lens materials, lens care solutions, and wearing modalities, the rate of MK associated with contact lens wear remains unchanged (Stapleton, 2008). Bacterial keratitis (as opposed to fungal or protozoan infection) remains the most common form of corneal infection that contact lens practitioners will encounter (Figure 1), with the most common organism being Pseudomonas aeruginosa.
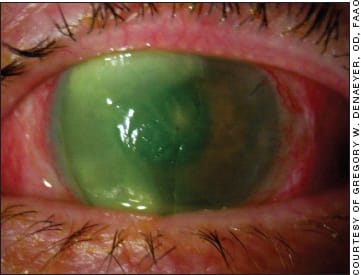
Figure 1. Severe bacterial corneal ulcer.
A Controversial Treatment
Microbial keratitis is the third leading cause of corneal inflammation, following trachoma and Herpes simplex viral eye disease (Wilhelmus, 2002). The inflammation that accompanies bacterial keratitis and other MK accounts for much of the edematous, infiltrative, and necrotizing changes associated with the event. The host response to microbial invasion involves the recruitment and activation of neutrophils and other leukocytes to the site of microbial proliferation. Corticosteroids are widely available and effective for down-regulating this response, which can ultimately modify wound healing in the infected and inflamed corneal tissue.
However, the use of corticosteroids in the treatment of bacterial keratitis has been controversial for more than 50 years. There are two sides to the argument. Proponents of their use strongly believe that they reduce tissue damage associated with the immune response to infection. Those opposed to their use believe that they may enhance infection, promote recurrence, or delay wound healing. At this point in time, both sides of the argument are acceptable according to the American Academy of Ophthalmology's Preferred Practice Pattern (Srinivasan, 2009; Matoba, 2000), and thus both practices can be medically and ethically justified.
The controversy over corticosteroid use in bacterial keratitis applies only to active infectious processes with replicating bacterial organisms within the corneal tissue. This is entirely different from the so-called “sterile” corneal ulcers in which the disease process is an inflammatory response to an antigen that may be microbial or of microbial origin. For example, contact lens-associated inflammatory events such as contact lens acute red eye (CLARE) and contact lens peripheral ulcers (CLPUs) are examples of infiltrative complications that have been associated with high levels of gram negative and gram positive organisms on the lens surfaces. Although these complications can often be treated by simply removing the stimulus to inflammation (the lens), concomitant antibiotic and corticosteroid treatment can be used in situations in which the inflammation is severe and faster resolution is desired.
Looking for Answers
For treating corneal infections, what is the evidence that either side is correct? Limited literature is available on this topic and very few clinical trials have been performed. There are only two published clinical trials that have very small sample sizes with inconclusive results (Carmichael, 1990; Srinivasan, 2009). The most recently published study by Srinivasan and colleagues was a small pilot study to rule out a large effect of steroid use and to assist in the planning and sample size calculations for a much larger trial on this topic.
In 1990, Carmichael and colleagues published a study of 40 patients in South Africa who had bacterial corneal ulcers. All patients were aggressively treated with combination antibiotic therapy. After such treatment for 24 hours, one group (21 eyes) was randomized to add dexamethosone 0.1% four times daily to the treatment regimen until healing was complete. The primary assessment was the resultant best-corrected visual acuity, but healing rate and complications were also assessed. Complications were similar between the groups (eight in the steroid group and 10 in the non-steroid group) and included perforation, corneal thinning, recurrent infection, persistent epithelial defect, and epithelial breakdown in both groups. Healing rates were also similar between the groups, calculated to be 0.36mm2/day for the steroid group and 0.30mm2/day for the non-steroid group. Ultimately, the authors were not able to demonstrate any difference in visual outcomes between the two groups.
In 2009, Srinivasan et al published their pilot randomized clinical trial on 42 patients in India who had culture confirmed bacterial keratitis to assess whether adjunctive topical corticosteroid use improved outcomes. If no difference was found, then they determined the feasibility and sample size required to conduct a larger trial to answer this question. All patients received topical moxifloxacin (Vigamox, Alcon), and after at least 48 hours, patients were randomized to either topical prednisolone phosphate 1% or a placebo sodium chloride drop used four times per day for one week, followed by two times per day for one week, then once a day for one week, and then stopped. All patients continued to receive moxifloxacin every two hours while awake until re-epithelialization occurred, then four times per day. They found a statistically significant delay in re-epithelialization in the steroid group (average times: 6.3 days in the placebo group and 8.6 days in the steroid group). However, this delayed epithelialization did not result in any statistically significant differences in best-corrected spectacle acuity or infiltrate/scar size at three weeks or three months after enrollment between the groups. In fact, although not statistically different, the steroid group was associated with a nearly two-line improvement in best-corrected acuity at three weeks and a nearly one-line improvement by three months. Compared to placebo, the steroid group also had a greater decrease in infiltrate/scar size at three weeks and three months (not statistically significant).
Answers in Sight?
The Steroids for Corneal Ulcers Trial (SCUT; NCT00324168) that is currently ongoing was spun from the 2009 Srinivasan preliminary trial previously mentioned. SCUT is run out of the Proctor Foundation at the University of California, San Francisco with two United States locations and three locations in India contributing patients. The study started in 2006, and 500 cases are expected to be enrolled and followed with an estimated completion date coming up very soon (February 2011). The same protocol as the Srinivasan et al study is being implemented.
The larger sample size should be able to provide the definitive answer as to whether the non-significant associations between steroid use and improved visual acuity and smaller scar size as noted in the pilot study will be realized. Stay tuned! CLS
To obtain references for this article, please visit http://www.clspectrum.com/references.asp and click on document #182.
Dr. Szczotka-Flynn is an associate professor at the Case Western Reserve University Dept. of Ophthalmology & Visual Sciences and is director of the Contact Lens Service at University Hospitals Case Medical Center. She is a consultant or advisor to B+L and Inspire Pharmaceuticals and has received research funding from Alcon and Vistakon. You can reach her at loretta.szczotka@UHhospitals.org.