


THE CORNEA
A Closer Look at Corneal Stem Cells
Early intervention by practitioners can prevent and aid treatment of limbal stem cell deficiency.
By Katherine M. Mastrota, MS, OD, FAAO, & William Townsend, OD, FAAO
We would imagine that similar to most of us, you confidently assure uncomfortable patients who have a corneal abrasion that the injury will heal relatively quickly with a good chance that their vision will be uncompromised. We daily take for granted the remarkable architecture and exquisite processes that create and regenerate the optically clear cornea.
How does the cornea maintain itself? How do superficial corneal abrasions heal? Why does corneal staining go away? Why can a cornea become vascularized?
Corneal Anatomy Review
To better consider the above questions, a brief review of corneal anatomy is in order. A full-thickness cross-section of the human cornea would show (anterior to posterior) the five- to seven-cell-layered epithelium and the three layers of stroma, which include Bowman's layer, the lamellar stroma with its resident keratocytes (which occupy more than 90 percent of the corneal tissue) and Descemet's membrane, which is the thickened basement membrane of the corneal endothelium. The endothelium is a low, cuboidal monolayer of cells that borders the anterior chamber.
The limbal epithelium is structurally similar to the corneal epithelium. It is a transitional barrier, protecting the cornea from encroachment by conjunctival epithelial cells and vasculature. Unlike the cornea, however, melanocytes and Langerhan's cells frequently can be found interspersed between the cells of the limbal epithelium. Additionally, undulating extensions of the basal surface (palisades of Vogt) insert into an underlying matrix. Evidence strongly indicates that in humans, corneal stem cells are concentrated along the bottom of the epithelial papillae that form the limbal palisades of Vogt (Lavker et al, 2004; Dua et al, 2005; Daniels et al, 2006; Li et al, 2007). Corneal stem cells are not equally distributed in all species; there is good evidence that in mice, stem cells reside in the central cornea and migrate toward the limbus (Majo et al, 2008).
Stem Cell Primer
The ability to continuously replace various types of cells as they are damaged or lost to normal turnover is essential to the health of any multicellular organism. Stem cells possess two unique attributes. They are unspecialized cells capable of uninterruptedly replicating themselves through cell division over the lifespan of an organism. Secondly, under specific physiologic or experimental conditions, they can be prompted to become tissue- or organ-specific cells (Majo et al, 2008). More explicitly, stem cells can generate daughter cells identical to their mother (self-renewal) as well as produce progeny with more restricted potential (differentiated cells) (Lanza, 2009). In adult organisms, stem cells are responsible for regulating cell populations in tissues that undergo continuous turnover (Fuchs and Segre, 2000).
During the first few hours after a human egg is fertilized, it divides into multiple identical cells that are said to be totipotent (Figure 1). These cells have the capacity to form an entire organism. At approximately four days after fertilization, after several cycles of cell division, pluripotent cells can give rise to most, but not all, of the tissues essential for fetal development. Further division yields even more specialized cells, multipotent cells, that have a specific function. For instance, hematopoetic multipotent stem cells can give rise to leukocytes, erythrocytes, and platelets. Unipotent stem cells are cells in adult organisms that are capable of differentiating along only one lineage (producing one type of tissue) (Fuchs and Segre, 2000).
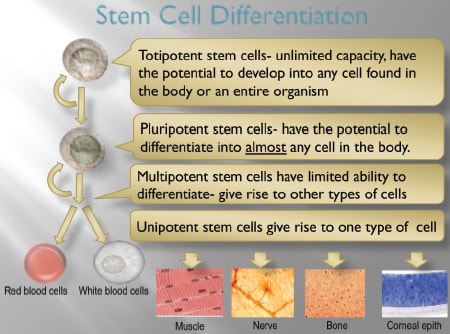
Figure 1. Different types of stem cells and their functions.
Stem Cells and the Cornea
The adult stem cell population of the corneal epithelium is one of the better-understood stem cell systems in the body. Because of their easily accessible location, limbal stem cells provide an excellent site for studying stem cell anatomy and function (Daniels et al, 2006).
Corneal stem cells are responsible for replacing epithelial cells lost in the normal turnover of the corneal epithelium and for replacing damaged epithelium (Daniels et al, 2006). Corneal limbal stem cells can divide either symmetrically to produce two daughter stem cells or asymmetrically to create one daughter stem cell and one progenitor (or transient amplifying) cell. Transient amplifying cells, which have only limited proliferative capacity, migrate centripetally from the limbus and vertically from the basal epithelial layers forward, eventually giving rise to terminally differentiated cells (Lehrer et al, 1998; Dua et al, 1994). Terminally differentiated cells are highly specialized and have no proliferative capacity (Sun and Lavker, 2004; German et al, 2006). The apical layers of the corneal epithelium are made of terminally differentiated cells. When the apical corneal epithelial cells reach the end of their life cycle, they are sloughed from the corneal surface and replaced by underlying maturing cells.
Thoft and Friend (1983) proposed that a dynamic equilibrium exists among the centripetal movement of epithelial cells, the differentiation of basal cells into superficial cells, and the desquamation of epithelial cells from the corneal surface (The XYZ Theory of Thoft). During the healing of corneal epithelial wounds, sheets of epithelial cells migrate centripetally from the limbus and circumferentially along the limbus to cover the defect. As an interesting aside, the whorled or vortex pattern (similar to that seen in corneal verticillata) observed in hurricane/blizzard keratopathy probably reflects the path taken by corneal epithelial cells during normal replicative turnover as they migrate from the limbus to the center of the cornea. Hurricane keratopathy is thought to be evidence of chronic epithelial breakdown and healing and can be observed in corneal graft patients (and rarely contact lens patients) where corneal epithelial cell turnover is exaggerated (Dua et al, 1993).
In the cornea, limbal stem cell deficiency (LSCD) can be primary, related to an insufficient stromal microenvironment to support stem cell function such as in congenital disorders (e.g. aniridia), or a manifestation of one of the ectodermal dysplasia syndromes. Secondary stem cell disorders develop from external factors that damage stem cells with insult over time. Collagen-vascular diseases; chemical, thermal, or radiation injury; medication toxicity; multiple ocular surgeries, chronic ocular surface inflammation such as in rosacea, staph marginal disease, or extensive microbial infection can all result in partial or total LSCD, which in turn can result in conjunctivalization of the corneal surface (Puangsricharem and Tseng, 1995; Sridhar et al, 2001). LSCD can also result from soft lens wear, either from the mechanical friction on the limbus or from lens-induced hypoxia.
Impaired function of corneal epithelial stem cells/limbal architecture is responsible for corneal surface damage and is clinically characterized by a dull and irregular corneal reflex, recurrent epithelial defects, neovascularization, corneal opacity, and conjunctivalization. Conjunctivalized corneal surfaces stain “late” with fluorescein, as conjunctival epithelium is more permeable compared to corneal epithelium. In partial stem cell deficiency, a clear line of demarcation can sometimes be seen between the corneal and conjunctival phenotype of cells. Subjectively this is represented by mild ocular irritation or foreign body sensation, recurrent episodes of pain (epithelial breakdown), lacrimation, photophobia, redness, and reduced acuity. A recent case series of presumed contact lens-related LSCD suggests that focal LSCD can present with varying manifestations and that it may be more common than currently reported (Jeng et al, 2011). The authors included patients whose clinical presentation was suggestive of LSCD, that is as dull, opaque-appearing epithelium with a “streaming” appearance, sometimes associated with superficial vascularization, emanating from the limbus.
Corneal stem cell deficiency can be best confirmed histologically by the use of impression cytology, which can detect goblet cell-containing conjunctival epithelium on the corneal surface. Recent studies demonstrate the potential for identifying limbal stem cells using confocal microscopy (Hong et al, 2011).
Case Report
A 15-year-old female presented to our office complaining of bilateral pain and photophobia. She had worn soft traditional hydrogel lenses for four years. The patient admits that she frequently wears the daily wear contact lenses on an extended wear basis for days and occasionally weeks at a time.
The patient's presenting visual acuities with contact lenses were OD 20/30 and OS 20/60. External examination revealed bilateral pannus spreading downward from the anterior limbus; vascularization was much more extensive in the left eye, extending close to the visual axis (Figures 2 and 3). After removing the contact lenses, we noted a coarse punctate keratitis that was more pronounced in the left eye (Figure 4). We also found significant superior limbal edema OD and OS.
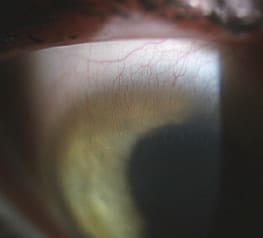
Figure 2. Patient's pannus OD.

Figure 3. Patient's pannus OS.
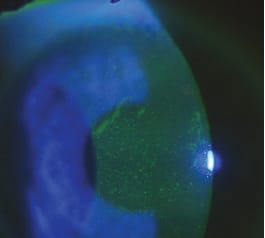
Figure 4. Patient's punctate keratitis.
We initially diagnosed limbal stem cell loss secondary to chronic hypoxia and lens over wear. Our diagnosis was based on clinical appearance and history. We instructed the patient to discontinue contact lens wear and prescribed a topical 1% steroid suspension every four hours OD and OS. One week later, the patient returned to our office wearing her lenses. When we asked why, she said that she “had to wear them” for softball practice. The appearance of the patient's cornea was unchanged and there was no improvement in any facet of her condition.
We referred the patient for a corneal consult to determine the feasibility of surgical intervention. In many cases this condition responds well to stem cell transplantation. The specialist recommended that we delay surgery, and that the patient discontinue all contact lens wear. We have seen significant regression of the pannus and improvement in the keratitis in the right eye. Unfortunately we have seen very little improvement in the left eye. This patient, an avid athlete, is able to wear high-Dk contact lenses on a very limited basis, only for practice and games. Ultimately our patient may require a limbal stem cell transplant.
This case demonstrates the real potential for permanent ocular damage resulting from chronic abuse of contact lenses.
Fixing LSCD
Restoration of corneal epithelial stem cells is achievable by transplantation of corneal stem cells. Kenyon and Tseng published the first series of successful limbal stem cell transplants in 1989.
In conjunctival limbal autografting, the stem cell-containing limbal grafts are harvested from the healthy fellow eye of the patient and transplanted into the stem-cell-deficient eye. In comparison, conjunctival limbal allografting uses graft segments from living-relative eyes or even from cadaveric sources. Ex vivo stem cell expansion (cultured corneal epithelial cells) provides another source of stem cells for transplantation.
Perhaps one of the best means of dealing with limbal stem cell deficiency is preventing it. In cases of congenital conditions such aniridia, there is currently no therapy available.
Noncompliant contact lens wear continues to be one instance in which eyecare practitioners can impact the development of stem cell loss. Most contact lens-related stem cell changes occur in the superior cornea. Patient education is crucial, especially in individuals who are known to be noncompliant and chronic “abusers” of contact lens wear.
In cases related to contact lens wear, topical steroids are often effective treatment. In cases that are nonresponsive to steroid therapy, superficial keratectomy with conjunctival autograft from an unaffected sector of the affected cornea or from the fellow eye is often useful in resolving LSCD keratitis (Jeng et al, 2011).
Summary
Corneal limbal stem cell deficiency is a rare but potentially sight-threatening condition arising from congenital or acquired etiologies. It is important that practitioners recognize and treat it or refer the patient as early as possible in the course of this condition. Medical and surgical therapies are often successful in improving vision and reducing symptoms. New investigative and treatment modalities may allow us to make earlier diagnoses and to intervene earlier in the process. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #188.

|
Dr. Mastrota is secretary of the newly formed Ocular Surface Society of Optometry (OSSO). She is center director at the New York Office of Omni Eye Services and is a consultant to Allergan, AMO, B+L, Inspire, Noble Vision, and Cynacon Ocusoft. You can reach her at katherine-mastrota@msn.com. |

|
Dr. Townsend practices in Canyon, Texas and is an adjunct faculty member at UHCO. He is an advisor to TearLab Corporation, has received research funds from Alcon and B+L and is an advisory panel member of Alcon, B+L, and Inspire Pharmaceuticals. You can reach him at drbilltownsend@gmail.com. |