


LENS-RELATED DRY EYE
Dry Eye in Soft Contact Lens Wearers
A variety of tools are available to help you diagnose and manage this multifactorial condition.
By Heiko Pult, PhD, MSc, FAOO, FBCLA, FEAOO
Discomfort during contact lens wear is one of the major causes of discontinuation—approximately half of patients in the United Kingdom and three-quarters of those in the United States who drop out do so because of lens wear discomfort (Pritchard, 2001). The frequency of contact lens-related dry eye (CLRDE) is about 50 percent (Nichols et al, 2002; Begley et al, 2000b; Nichols and Sinnott, 2006), and it can be associated with reduced visual acuity and wearing comfort as well as an increased risk of ocular surface alterations and infection (Ladage et al, 2001).
CLRDE and Lens Material
Many soft contact lens materials are available. They can be hydrogel or silicone hydrogel (SiHy). In 2008, 36 percent of soft lenses were manufactured from SiHy (Morgan et al, 2010). This increased to 51 percent worldwide in 2010 (Morgan et al, 2011). Lens comfort depends on parameters such as water content, wettability, adsorption of proteins, modulus, and oxygen permeability (Sindt and Longmuir, 2007).
Dehydration changes the flexibility of the contact lens as well as its oxygen transmission and lens fit, which can affect lens comfort, visual quality, and the ocular surface (Dillehay, 2007). Because the bulk water content of contact lenses changes significantly only within the first 5 to 10 minutes on the eye (Brennan et al, 1987; Efron et al, 1987), lens surface dehydration is more important (Sindt and Longmuir, 2007).
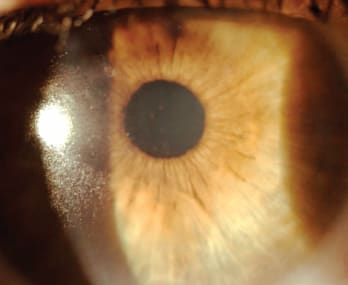
Figure 1. Poor tear film spreading and drying of a SiHy contact lens in a CLRDE patient.
Thinning of the pre-lens tear film (PLTF) depends on the quality and thickness of the lipid tear film layer (Cedarstaff and Tomlinson, 1983), which is disrupted by a contact lens (Sindt and Longmuir, 2007). Even though the PLTF thickness with SiHy contact lenses is similar to that with hydrogel contact lenses, the pre-lens breakup time is shorter for SiHy lenses (Nichols et al, 2005). During PLTF rupture, an evaporative-dehydration process starts that draws water through the lens and out of the post-lens tear film, leading to corneal staining (Fonn, 2007).
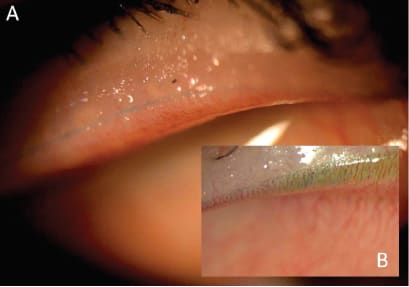
Figure 2. Line of Marx (A) versus lid wiper epitheliopathy (B).
Furthermore, symptoms of dryness are assumed to be closely related to the surface wettability (Figure 1) of a contact lens (Tonge et al, 2001). However, even though hydrogel lenses are known to have a better in-vitro wettability than SiHy lenses do (Lorentz et al, 2007), symptoms of dryness and discomfort in symptomatic hydrogel contact lens wearers have been reported to be reduced with SiHy lenses (Brennan et al, 2002; Long and McNally, 2006; Woods and Morgan, 2004; and others, full list available at www.clspectrum.com/references.asp).
Ionicity is important in the interaction between a contact lens and the tear film. A related concern is that ionic hydrogel materials attract too much protein because these proteins get denaturized if deposited on the contact lens surface (Senchyna et al, 2004). Denatured protein is related to contact lens complications such as giant papillary conjunctivitis (GPC) and inflammation, both of which are associated with symptoms of dry eye (Sindt and Longmuir, 2007). Although ionic materials are more likely to deposit increased amounts of protein, non-ionic polymers will deposit more lipid, impacting the PLTF (Jones et al, 1997a). SiHy materials demonstrate reduced protein deposition, but they have a greater percentage of denatured lysozyme (Luensmann et al, 2010). Additionally, some patients who previously wore hydrogel lenses may experience more lipid deposition with SiHy lenses (Lorentz and Jones, 2007). However, rubbing and rinsing the lenses can remove lipid and protein from the lens surface (Sindt and Longmuir, 2007). Regular lens replacement, in addition to appropriate lens hygiene, will result in improved clinical performance (Jones et al, 1997b; Jones et al, 1997a).
The success of a contact lens material and the impact of these external forces are governed by the mechanical properties of the material. Stiffer lenses are associated with general lens awareness, mechanically induced GPC, conjunctival flaps (Santodomingo-Rubido et al, 2008), and superior epithelial arcuate defects (Sindt and Longmuir, 2007). The further development of silicone hydrogels to allow reduced modulus while still maintaining excellent oxygen permeability or a greater spectrum of lens parameters may be of benefit (Schafer, 2006).
A sufficient level of available oxygen is fundamental for healthy eyes and, therefore, for successful contact lens wear (Dillehay, 2007). It is established that clinical signs of hypoxia with SiHy wear improve concurrently with improvements in patient symptoms of comfort and dryness (Dillehay, 2007). Expectedly, symptoms of dryness and discomfort decrease when refitting hydrogel lens wearers with SiHy lenses (Brennan et al, 2002; Long and McNally, 2006; Woods and Morgan, 2004; and others).
Contact Lens Solutions
Contact lens solutions remove proteins by using negatively charged molecules that pull the positively charged proteins from the lens surface. Alternatively, enhancing surface wettability can protect a lens from deposition. Removing lenses from the packaging and soaking them in certain types of contact lens solution may further increase the initial lens wettability (Sindt and Longmuir, 2007). For example, the latest generation of daily disposable lenses exhibit significantly different wettabilities, some of which are directly due to components of the packaging solutions (Menzies et al, 2010). However, some solution-related disinfecting agents are related to contact lens dryness and should be avoided (Lievens et al, 2006).
Diagnosis of Contact Lens-Related Dry Eye
Because dry eye symptoms are more distinct compared to its ocular signs, a good history is crucial in the diagnosis of CLRDE. Many questionnaires are available, such as the Contact Lens Dry Eye Questionnaire (CLDEQ) (Nichols et al, 2002; Begley et al, 2001; Begley et al, 2000b), the Dry Eye Questionnaire (DEQ) (Begley et al, 2001), the CLDEQ-8 (Chalmers et al, 2010; Chalmers et al, 2009), the Impact of Dry Eye on Everyday Life questionnaire (IDEEL) (Rajagopalan et al, 2005), McMonnies Dry Eye Index (McMonnies and Ho, 1987b; McMonnies and Ho, 1987a; McMonnies, 1986; and others), and the Ocular Surface Disease Index (OSDI) (Nichols and Smith, 2002; Schiffman et al, 2000; Vitale et al, 2004).
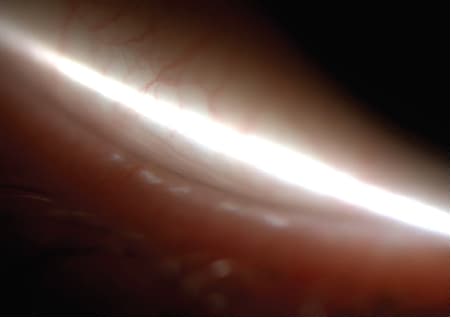
Figure 3. Temporal LIPCOF grade 2.
The McMonnies Dry Eye Index is probably the most noted questionnaire and is more useful for dry eye diagnosis than as a measurement of dry eye symptoms (Gothwal et al, 2010). It considers epidemiological risk factors, the frequency of symptoms of ocular irritation, and sensitivity to environmental triggers. Even though developed for non-lens wearers, it was suggested to also be useful in contact lens wearers (Michel et al, 2009); others reported reduced predictive abilities (sensitivity = 34 percent and specificity = 86 percent) (Nichols et al, 2002).
Even though the OSDI was developed more recently to grade the severity of dry eye as well as for diagnosis in non-contact lens wearers, it was also successfully used in contact lens studies (sensitivity = 76.9 percent and specificity = 90.0 percent [naïve lens wearers (Pult et al, 2009)]) (Versura et al, 2010a; McDonald et al, 2009; Hom and Bruce, 2009). It is notable among other ocular surface disease questionnaires for having undergone psychometric testing and having been accepted by the U.S. Food and Drug Administration (FDA) as an outcome measure for use in dry eye trials (Sall et al, 2000; Schiffman et al, 2000; Stevenson et al, 2000). This instrument has three sub-scales that sequentially ask for symptoms of ocular irritation, the impact on vision-related functioning, and environmental triggers of dry eye syndrome.
The CLDEQ diagnoses dry eye in contact lens wearers by a dichotomous outcome (sensitivity = 61 percent and specificity = 83 percent) (Nichols et al, 2002). It focuses on ocular surface symptoms rather than on presumed risk factors for dry eye syndrome. There are nine symptom sub-scales; each sub-scale asks about the frequency of the symptom, followed by three questions concerning the intensity of the symptom at different times of day to examine diurnal fluctuations in symptoms (Nichols et al, 2002; Begley et al, 2000b; Begley et al, 2001). The difference with the CLDEQ (companion to the DEQ) is that it anchors to the overall dry eye status via the question “Do you think you have dry eyes?” and uses that to stratify. Most of the other questionnaires don't have this internal anchor. The CLDEQ is also available in a short form (three questions plus sub-scales).
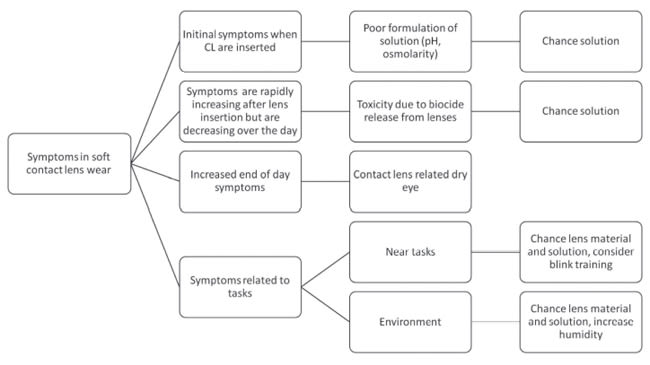
Figure 4. Evaluation algorithm of contact lens-related symptoms.
To measure overall opinion of contact lens performance, the CLDEQ-8, which includes an anchoring question on “Overall Opinion,” was developed (Chalmers et al, 2010; Chalmers et al, 2009). The CLDEQ-8 score was reported to significantly reflect baseline status and change of overall opinion regarding contact lens performance and could be an efficient outcome measure in clinical trials and practice (Chalmers et al, 2010; Chalmers et al, 2009).
Many objective tests are used in clinical practice, but their efficacy in predicting CLRDE is controversial (Glasson et al, 2003; Pult et al, 2008; Nichols et al, 2004b). Tear film measurements are mostly not applied in the normal routine of contact lens after-care because lenses have to be removed for some time prior to measurements (Johnson and Murphy, 2005); in some studies, patients were even asked to remove lenses one day prior to evaluations (Glasson et al, 2003). However, the measurement of PLTF thinning might be an option in experienced lens wearers. While Hom and Bruce (2009) and Nichols et al (2006) found a good relationship between CLRDE symptoms and PLTF thinning (using specular reflection and a thickness-dependent fringe imaging interferometer, respectively), others suggested that PLTF thinning is not a good predictor of CLRDE (using the TearScope Plus [Keeler Ltd., Windsor, UK], Pult et al, 2008).
Even though a battery of tests can be applied in naïve contact lens wearers (before fitting lenses), non-invasive breakup time (NIBUT) (sensitivity = 61.5 percent and specificity = 10.0 percent) and lid parallel conjunctival fold (LIPCOF) sum (sensitivity = 69.2 percent and specificity = 90.0 percent) were reported to be the only significant discriminators of later CLRDE in naïve lens wearers (Pult et al, 2009).
However, the investigation into more or less uncommon tests such as lid wiper epitheliopathy (LWE) (Korb et al, 2002), LIPCOFs (Höh et al, 1995; Pult et al, 2009; Pult et al, 2008) and tear osmolarity (Benelli et al, 2010; Messmer et al, 2010; Tomlinson et al, 2010; and others) as well as test combinations demonstrated promising results.
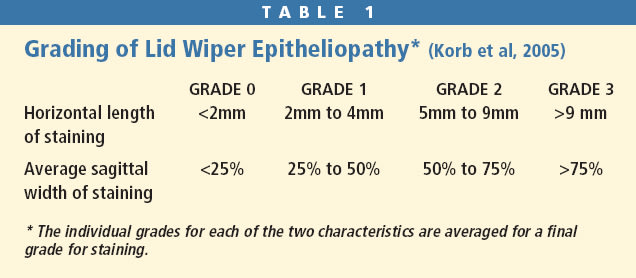
LWE is a clinically observable alteration in the epithelium of the advancing lid margin, called the lid wiper. In patients who have dry eye, the tear film is insufficient to separate the ocular surface and lid wiper (Korb et al, 2005), hence the lid wiper is subjected to trauma during the entire lid movement (Korb et al, 2002; Korb et al, 2005). LWE is a significant discriminator of CLRDE (sensitivity = 87.0 percent, specificity = 42.1 percent) (Pult et al, 2008).
LWE is visible using a combination of instilled 1% lissamine green (or rose bengal) and 2% fluorescein, and is evaluated for the upper lid. A second instillation of both dyes should be carried out after 5 minutes (Korb et al, 2006). LWE is classified by width and length (Table 1) (Korb et al, 2002; Korb et al, 2005). Take care to differentiate between staining associated with Marx's line (Pult et al, 2010a; Korb and Blackie, 2010) and that from staining of the lid wiper (Korb et al, 2002; Korb et al, 2005) (Figure 2).
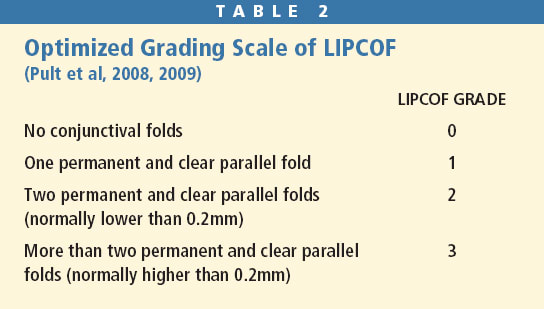
LIPCOFs are sub-clinical folds in the lateral, lower quadrant of the bulbar conjunctiva that are parallel to the lower lid margin (Höh et al, 1995; Sickenberger et al, 2000; Schirra et al, 1998; Pult et al, 2008) and are easily observable by slit lamp (Figure 3). LIPCOFs are evaluated in the area perpendicular to the temporal and nasal limbus on the bulbar conjunctiva above the lower lid with a slit lamp microscope using 18x to 27x magnification as necessary, and are classified by number of folds (Table 2) (Pult et al, 2009; Pult et al, 2008). The sum of temporal and nasal LIPCOFs has a higher predictive value compared to regional LIPCOF scores (sensitivity = 82.6 percent, specificity = 84.1 percent) (Pult et al, 2008). The combined LIPCOF score (LIPCOF Sum) is calculated by adding together the temporal and the nasal LIPCOF grade (Pult et al, 2008). Take care to differentiate between parallel, permanent conjunctival folds (LIPCOFs) and disrupted micro-folds and to use the correct technique (no fluorescein, no contact lens, primary gaze) and area of observation (Pult et al, 2009; Pult et al, 2008).
LIPCOFs are assumed to result from mechanical forces in blinks in dry eye patients, since LWE and LIPCOF are significantly correlated and LWE and LIPCOF are also related to mucin quantity (Berry et al, 2008). Both tests can be performed immediately after lens removal (Pult et al, 2008; Korb et al, 2002).

Figure 5. Obstructive meibomian gland dysfunction.
The International Dry Eye Workshop (DEWS) (2007) recognized the role of tear hyperosmolarity in dry eye. Tomlinson et al (2006) concluded that tear hyperosmolarity, defined by a referent of 316 mOsmol/L, is superior in overall accuracy to any other single test for dry eye diagnosis. Khanal et al (2008) concluded that the measurement of the tear osmolarity is the best single test for the diagnosis of dry eye (sensitivity = 78 percent and specificity = 78 percent [non-lens wearers]).
The TearLab Osmolarity Test (TearLab Corp.) has now enabled a possibility of measuring tear film osmolarity in clinical practice. Many studies have discussed its value in dry eye diagnosis (Versura et al, 2010b; Tomlinson et al, 2010; Sullivan et al, 2010; and others). The “TearLab Research Guide” recommends measuring osmolarity 10 to 15 minutes before application or after removal of contact lenses and to measure the effect of lens wear with the lens on the eye. The usefulness of evaluating tear osmolarity in contact lens wearers is obvious, but still not fully investigated (Landers et al, 2011).
Combining different tests can increase predictive ability of dry eye (Sullivan et al, 2010; Begley et al, 2000a; Glasson et al, 2003). The Contact Lens Dry Eye Index (CLIDE-Index), a combination of temporal and nasal LIPCOF with patient symptoms (CLDEQ questions 2 through 5 [dryness minus grittiness) was reported to screen and measure the dry eye state of experienced contact lens wearers (sensitivity = 87 percent and specificity = 87 percent) (Pult et al, 2010b). Glasson et al (2003) suggested a combination of the McMonnies dry eye questionnaire with tear film stability and tear film volume to detect symptomatic experienced lens wearers (sensitivity = 87 percent and specificity = 50 percent). The combination of the OSDI with temporal and nasal LIP-COF and NIBUT (named the Contact-Lens-Predicting-Test [P-Test]) showed good predictive ability (sensitivity = 92 percent and specificity = 90 percent) (Pult et al, 2009) of later CLRDE symptoms in naïve contact lens wearers.
Figure 4 shows an evaluation algorithm of CLRDE symptoms.
Treatment Options in CLRDE
Even though not all characteristics of SiHy contact lenses are superior to those of traditional hydrogel contact lenses, refitting symptomatic hydrogel lens wearers into SiHy lenses is worth a try because they usually improve CLRDE symptoms (Chalmers et al, 2008; Schafer et al, 2007). Also, fitting criteria and different lens designs have to be addressed (Dumbleton et al, 2002; Santodomingo-Rubido and Rubido-Crespo, 2008).
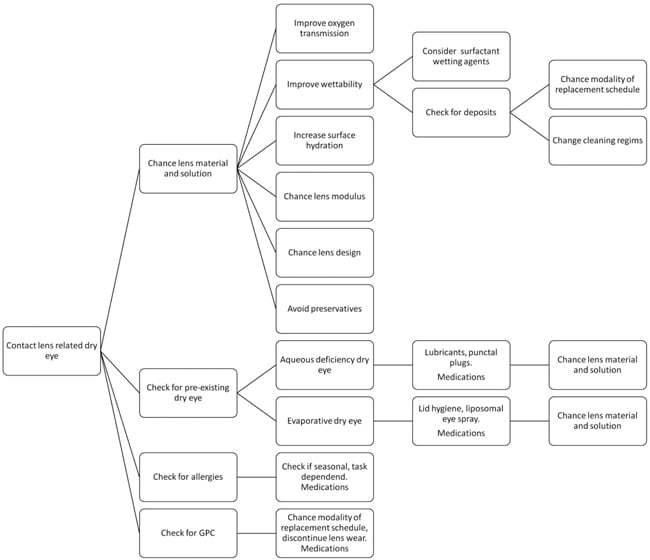
Figure 6. Treatment strategies in CLRDE.
An additional option is to improve contact lens wettability with rewetting drops and appropriate contact lens care regimens (Sindt and Longmuir, 2007; Subbaraman et al, 2006). Artificial tears containing hyaluronic acid (Johnson et al, 2006) or a surrogate (Springs, 2010), hypo-osmotic eye-drops (Stahl et al, 2010) or liposomal eye sprays (Craig et al, 2010; Dausch et al, 2006), and possibly nutrition (Rosenberg and Asbell, 2010) can help improve symptoms, ocular signs, and the tear film.
Many symptomatic lens wearers demonstrate pre-existing dry eye (Pult et al, 2009; Sindt and Longmuir, 2007). Therefore, a good history and proper evaluation of the tear film and the ocular surface are essential. Besides lipid anomalies and primary aqueous tear deficiency, ocular allergies must be addressed because their symptoms overlap with dry eye symptoms (Sindt and Longmuir, 2007). Especially consider dysfunction of the meibomian glands (MGD) because MGD might be the most common cause of dry eye (Foulks and Bron, 2003; Knop et al, 2009; Nichols et al, 2011) (Figure 5). Unfortunately, the role of the lid margins is often underestimated
(Knop et al, 2010). Consistent application of warm and moist compresses followed by lid massage and lid hygiene can improve dry eye status remarkably (Jackson, 2008; Sindt and Longmuir, 2007) in such patients.
Figure 6 shows a chart of treatment strategies for CLRDE.
Conclusion
Dry eye symptoms in contact lens wearers are multi-factorial. Pre-existing dry eye states should be addressed in managing CLRDE. New objective tests such as LWE and LIPCOF might be useful in clinical practice because they can be performed easily, without additional equipment, and immediately after lens removal. The best option to evaluate the dry eye status of naïve and experienced contact lens wearers is with a combination of objective tests and questionnaires. Refitting symptomatic hydrogel contact lens wearers with SiHy lenses can help reduce dry eye symptoms in most patients. The additional avoidance of preservatives and use of wetting agents and continuous lubrication of the ocular surface is promising. CLS
To obtain references for this article, please visit http://www.clspectrum.com/references.asp and click on document #188.

| Dr. Pult is an optometrist with about 15 years of experience in clinical practice as well as in clinical science. He completed his PhD in 2008 at the School of Optometry and Vision Sciences, Cardiff University, UK, where he is an honorary research fellow and member of the Contact Lens and Anterior Eye Research (CLEAR) Unit. His research interests are vision, tear film, cornea, and contact lenses. |