


Reader and Industry Forum
Imaging the Structure of the Meibomian Glands
By Sruthi Srinivasan, PhD, BS Optom, FAAO; Luigina Sorbara, OD, MSc, FAAO (Dip CL); Lyndon W. Jones, PhD, FCOptoM, FAAO (Dip CL); & Wolfgang Sickenberger, Prof, MSc Optom, Dipl Ing (FH) AO
The outermost layer of the tear film is composed of lipids, which are produced by the meibomian glands (MGs). MGs are tubuloacinar, holocrine glands that produce and secrete meibum (Bron and Tiffany 2004; Bron et al, 2004). Meibum of the appropriate quality and quantity is necessary for a healthy ocular surface, as the functions of the lipid layer include slowing evaporation of the aqueous tear components, enhancing tear film spreading and stability, preventing contamination of the tear film by sebum, preventing spill-over of tears from the lid margin, and closing the opposed lid margins during sleep (Gilbard et al, 1989; Gilbard 1999; Goto et al, 2003).
Meibum also contributes to providing a smooth optical surface at the air-tear interface, allowing for optimal vision (Mathers 1993; Millar et al, 2006). The contents of the MGs can easily be expressed with mild lid pressure immediately above or below the lash line.
A Need for MG Assessment
One of the main causes of dry eye is an abnormality of the meibum-secreting glands, which is termed meibomian gland dysfunction (MGD) (Mathers et al, 1993; Lemp, 1995; Goto, et al, 2003). MGD is a common clinical condition and is a major cause of evaporative dry eye, resulting in ocular discomfort, visual disturbance, and contact lens intolerance. Hence, a routine evaluation of the MGs and lipid layer is vital.
In a typical clinical setting, lid and lid margin evaluation is often performed with slit lamp biomicroscopy (Bron et al, 1991). But visualization of the MG structures is often not clear when a slit lamp is used in isolation; it may be necessary to include trans-illumination of the lids to clearly view the entire length of the MG (Robin et al, 1985).
To date, the only method available for the assessment of MG structure is meibography (Jester et al, 1982; Mathers et al, 1991; Mathers et al, 1994; Nichols et al, 2005). This technique is primarily regarded as a laboratory-specific procedure used by researchers for MG dropout assessment in subjects who have MGD; techniques used to evaluate MG structure and the lipid layer, such as meibography, tear interferometry (Yokoi et al, 1996), and meibometry (Chew et al, 1993; Yokoi et al, 1999; Komuro et al, 2002), are thought to occur only in “specialist” dry eye research laboratories.
More Accessible Meibography
Meibography was first introduced in the 1970s when Jester and coworkers pioneered the use of infrared (IR) light to transilluminate the lid, allowing easy observation of the glands (Jester et al, 1982). This was updated by Mathers and colleagues in the 1990s, who used an IR CCD video camera (Mathers et al, 1991; Mathers et al, 1994).
The Keratograph 4 (Oculus) is a non-contact device designed to provide a variety of non-contact corneal imaging and contact lens assessment tools, including placido ring-based corneal topography, fluorescein fit assessment of GP contact lenses, tear film breakup time, inferior tear meniscus height, pupillometry, and calculated oxygen transmissibility profiles.
In addition to these measurements, the availability of the IR illumination system (at 880nm) permits the device to capture both video and still images of the MGs within both the upper and lower lids with lid eversion (Figures 1 and 2). The videos can be played as .avi files, easily saved, and exported to any external drive. There is no calibration or initial preparation required to operate this form of imaging, and the device enables clear visualization of the MG structures with minimal training.
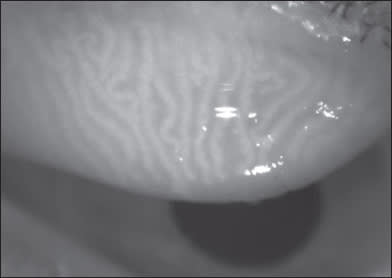
Figure 1. Meibography of the upper lid using Oculus Keratograph 4.

Figure 2. Meibography of the lower lid using Oculus Keratograph 4.
Work is ongoing to determine whether these images can be linked to patients who have MGD, aiding in its early diagnosis, and whether the appearance of the images changes following standard treatment procedures such as lid scrubs and warm compresses.
Multi-functional devices such as the Oculus Keratograph 4 provide eyecare practitioners with space-saving options within their practices. It is likely that many companies will continue to release such devices that use a single platform to provide multiple testing options. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #188.
Dr. Srinivasan is a research assistant professor at the School of Optometry, University of Waterloo, Canada. She is actively involved in research at the Centre for Contact Lens Research (CCLR) at the University of Waterloo. Dr. Sorbara is an associate professor at the University of Waterloo, Canada. She is actively involved in research at the CCLR. Her current research interests are in specialty contact lens designs, corneal topography, fluorophotometry, and clinical trials involving new lens materials, etc. Dr. Jones is director of the CCLR and a professor at the School of Optometry at the University of Waterloo. He has also received lectureship honoraria from Alcon, Ciba Vision, CooperVision, and Johnson & Johnson. Dr. Sickenberger is professor and head of the course of Optometry and Vision Sciences at University of Applied Sciences Jena, Germany. He is clinical director of JenVis Research, an independent research institute at University of Applied Sciences, Jena, Germany. He has also received lectureship honoraria from Oculus in Wetzler, Germany. The CCLR has received research funding from Alcon, Allergan, AMO, B+L, Ciba Vision, CooperVision, Essilor, Johnson & Johnson, Menicon, OcuSense, Paragon, and Visioneering.