


Contact Lens Practice Pearls
A Matter of Scale

By John Mark Jackson, OD, MS, FAAO
As eyecare providers, we rely upon clinical measurements a great deal. Sometimes we have to “tweak” the instruments a bit to give us the data we really need.
Custom Scale for Severe Keratoconus
I recently examined a patient who has keratoconus that I have followed for about eight years. He has one of the most severe cones I have ever seen. He was scheduled for a corneal transplant in his right eye the following week, but he had lost his left lens and needed a replacement until it was time for a transplant in the left eye in a few months.
It had been about two years since we last saw him, so we essentially started from scratch. When we performed topography, it showed a steep central area as would be expected with keratoconus. But careful observation of the default tangential map (Figure 1) showed that the central cornea had the same color of red throughout, yet the rings were not showing consistent spacing, indicating that the curvature varied a lot in this area. A quick look at the scale revealed the problem: the default used a standard scale that maxed out at 50.00D, and the topographer was displaying any curvature of 50.00D or steeper as the same color of red. This masked the true pattern.
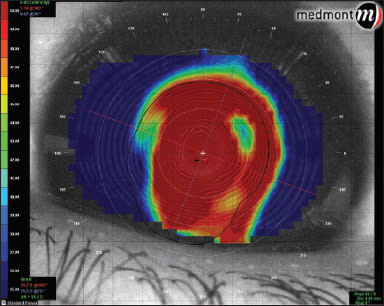
Figure 1. Our patient's topography map using the topographer's default scale.
A couple of clicks later and we had customized the scale for his cornea. The sim-K readings had a steep value of about 93.00D, so we set the upper limit of the scale at 95.00D. Figure 2 shows the adjusted scaling. The steepest area of the cone is much smaller and more centralized than it appears with the default scale.
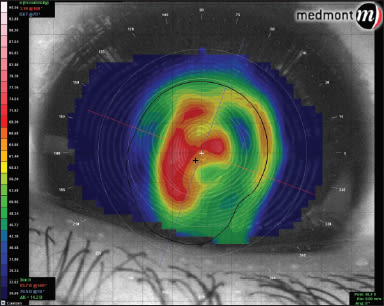
Figure 2. Topography map using customized scale.
Getting the Lens Right
We fit the patient with a traditional cone design because he had such a small central nipple cone. The parameters were: Rose K2 (Menicon/Blanchard Contact Lens), 4.50mm base curve, 8.7mm overall diameter, –39.00D. I was certain that the lab would get the power correct, but you should verify lenses before you call the patient. But how do you measure a –39.00D when the lensometer only goes up to –20.00D?
To do this, pair the minus lens with a plus lens. Ignoring thick lens optics for a moment, if you had a plus GP lens of +20.00D and held it back-to-back with the –39.00D, the combination should read about –19.00D. I doubt many offices have a +20.00D GP lens on hand, so you could add a few lower-power GP lenses together or you could also place a +20.00D loose trial lens against the lensometer stop and place your lens on top of that (Figure 3). Because of thick lens optics, neither of these methods will be perfect, but in our case we got within a 1.00D even with these high powers. CLS

Figure 3. A loose trial lens can help with verifying the power of an extremely high minus lens.
Dr. Jackson is an associate professor at Southern College of Optometry where he works in the Advanced Contact Lens Service, teaches courses in contact lenses, and performs clinical research. You can reach him at jjackson@sco.edu.