


IMPLEMENTING SCLERALS
Implementing Sclerals Into Your Practice
Fitting scleral lenses may seem intimidating at first, but with the right tools it's easier than you might think.
By Jeffrey Sonsino, OD, FAAO, & Marsha Malooley, OD, FAAO
Scleral lenses have seen a resurgence since the advent of GP materials and improved manufacturing techniques. Sclerals are readily available from several major laboratories with turnaround times of less than two weeks and practitioner-centered return policies. They are no more difficult to fit than any advanced GP lens design.
So why are more practitioners not fitting these lenses? We'll discuss scleral lens applications, how to get started, and some fitting pearls to make it easier for interested practitioners to take the plunge.
Scleral Lens Applications
Scleral lenses primarily have two uses: they act as a moisture chamber, and they provide optical clarity. Unlike traditional GP lenses, sclerals move very little, if at all, when fit properly. Capillary action keeps tears that are produced by the wearer adhered to both the lens and to the corneal epithelium. The classic example of this effect is making microscope slides with water. The droplet of water placed in between the microscope slide and the slide cover would keep for weeks without drying out.
The logical question to ask after hearing that the lenses do not move is: are they safe? The advent of highly oxygen-permeable materials has changed the landscape from when PMMA scleral lenses were first used in the 1940s. Modern GP scleral lenses are safe for wear. Even with little movement of the lens, oxygen diffusion keeps the corneal physiology operating within safe limits (Visser et al, 2007a).
In conditions such as Stevens-Johnson Syndrome, Sjögren's Syndrome, and chronic graft versus host disease, eyes are typically dry enough to perforate if not treated. Even patients on maximum medical therapy for dry eyes have significant morbidity that impairs quality of life (Ogawa et al, 1999).
A common use for scleral lenses is optical correction of an irregular cornea (Visser et al, 2007a; Visser et al, 2007b) (Figure 1). Sclerals can be used for advanced keratoconus, pellucid marginal degeneration, tilted grafts in post-penetrating keratoplasty, post-trauma, and even for Salzmann's Nodular Degeneration (Schornack and Patel, 2010; Schornack, 2009; Jacobs, 2008). When conventional corneal lenses inadequately correct vision, dislodge frequently, or compromise comfort, we move to a scleral contact lens.

Figure 1. Patient with a neurotrophic cornea, significant neovascularization, and partial tarsorrhaphy. A corneal GP lens was not stable enough to wear with proficiency. Best-corrected spectacle vision was 20/150. With a scleral lens, she achieved a stable 20/60.
Getting Started
The biggest step is taking the initiative to fit your first patient. You will find that scleral lenses are not as complicated as you may think. One lab consultant says that fitting scleral lenses is about vaulting the cornea and controlling bubbles. Although his statement is an over-simplification, it serves as a good starting point.
It is necessary to have the proper tools in place for fitting these large-diameter lenses, including preservative-free saline or artificial tears for lens application (Figure 2) and plungers to aid in application and removal. Some patients are able to balance the lens between their fingertips using the tripod technique for application (Figure 3). Others find it helpful to balance the lens on a plunger. It is recommended to have a variety of plungers available including large, ventilated, and non-ventilated plungers. We have found that larger plungers or smaller ventilated plungers are better for assisting in lens application; non-ventilated plungers may work better for removal. Handling scleral lenses can be initially awkward, but having access to a variety of plunger styles will increase your and your patients' success.

Figure 2. Patient applying a scleral lens. Because the chamber must be void of any trapped air, the patient fills the lens with either nonpreserved saline or nonpreserved artificial tears. The lens is kept horizontal, and the patient moves onto the lens for application.

Figure 3. The tripod technique allows a lens to be balanced among three fingers while full of solution.
Diagnostic lens fitting is essential to achieve a successful fit and to meet the fitting objectives of vaulting the central cornea, clearing the limbal region, and landing smoothly and evenly on the sclera without vessel impingement. Sagittal depth of the cornea is a key determinant in fitting; therefore, corneal topography is not as useful as it is in fitting other GP designs. Trial lenses will serve as your best topographer, allowing you to visualize the fitting relationship between the cornea and the posterior surface of the lens. Fitting guides and video tutorials are extremely helpful in diagnostic fitting and troubleshooting. Diagnostic lens sets are a financial investment, and selecting which set to purchase can be difficult. Consider starting with loaner sets to familiarize yourself with different lens designs before making a decision.
Be selective when choosing your first scleral contact lens patient. Choose a motivated patient who is willing to come back for multiple follow-up visits, but avoid the most complicated case in your office. Practice fitting techniques and lens handling on a family member or employee. It may not be a bad idea to practice lens application on yourself to see what your patients will experience. As with most specialty contact lens designs, there is a learning curve for fitting scleral lenses. Having a positive initial experience will encourage you down the road for future fittings.
Fitting Pearls
Once you decide to start fitting scleral lenses, the following fitting tips may help your fitting success rates:
• Using the consultation department at your laboratory is crucial for getting off the ground. The consultation department staff members have extensive experience fitting and troubleshooting scleral lens fits. We are both experienced scleral lens fitters who rely on the consultation departments heavily for individual cases. Never feel shy about using their skills!
• Scleral lenses are fit just like any advanced GP design. The basics of lens evaluation, inspection with sodium fluorescein, and over-refraction still apply. Diagnostic lens fitting (as opposed to empirical ordering) is much more important with sclerals.
• Initial scleral lens choices vary based on fitting philosophy, but a rule of thumb is 1.00D steeper than steep-K.
• Initial comfort is a big predictor of fit. If the lens is uncomfortable, a change is needed.
• Plasma treat all lenses. Plasma treatment is a technique used to rid the front surface of residues and imperfections. In your dry eye patients, front surface wetting will already be a problem. Take all steps to minimize lens desiccation.
• Technology is helpful, but not mandatory. Corneal topography can help highlight areas of concern. However, these areas will be visible with fluorescein inspection. Likewise, Dr. Sonsino performs anterior segment ocular coherence tomography (OCT) on all diagnostic fits. It serves as a great tool to better quantify corneal vault (Figure 4), but it is not absolutely necessary. Fluorescein pattern analysis will allow the same determination of fitting relationship between the cornea and the lens. Endothelial cell counts and morphology are helpful. At the 2005 World Cornea Congress, it was discussed that patients who have endothelial cell counts of less than 2,000 should not use scleral lenses. However, when the endothelial cell count falls below 2,000, there are signs of edema visible upon slit lamp examination.
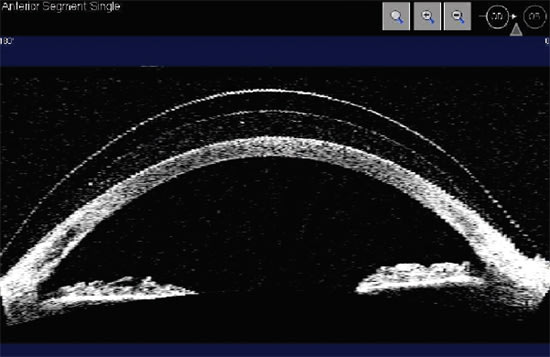
Figure 4. Anterior segment OCT image of a scleral lens on a patient who has graft versus host disease. Clearly visible are the front and back surfaces of the lens, the tear film, and the cornea. The fellow eye perforated due to dryness while on maximum medical therapy.
Easier Than You Think
Implementing scleral contact lenses into your practice can be very rewarding. Taking the first step can be scary; however, modern lens designs and in-office diagnostic fitting has revolutionized this lens modality. We hope our recommendations will help interested practitioners to get off the sidelines and into the scleral contact lens game. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #187.

|
Dr. Sonsino is an assistant professor at Vanderbilt Eye Institute where he is the chief of the optometry section. He is currently a candidate for Diplomate in Contact Lenses in the American Academy of Optometry. He is also the chair of the American Optometric Association's Anterior Segment Committee, co-editor of the Contact Lens Section Newsletter, and he has a financial interest in LVG, LLC, a low vision company. |

|
Dr. Malooley is part of a group MD/OD practice and serves as adjunct assistant professor of the Illinois College of Optometry in the Department of Community Based Education. She is a GP Lens Institute Advisory Committee member. |