


Contact Lens Case Reports
Fitting Post-HSV Corneas


By Patrick J. Caroline, FAAO, & Mark P. André, FAAO
Herpes simplex is a fairly common and usually unilateral viral infection of the cornea that can occur in any age group. Symptoms can include mild irritation, tearing, photophobia, and blurred vision. While the clinical presentation of the condition may vary (dendritic, disciform, geographic, or linear), the end result is often the same: a localized loss of stroma with marked regular and irregular corneal astigmatism.
Our patient is a 19-year-old female who suffered a herpes simplex infection to the right eye at age 6 with a recurrence at age 16. Since that time she has experienced blurred vision secondary to a diffuse central corneal scar (Figure 1). Her condition is currently controlled with acyclovir b.i.d. p.o., and slit lamp examination confirmed no active herpes infection. Visual acuity without correction was OD 20/100 and OS 20/15. Manifest refraction OD was +1.00 −5.50 x 125 VA 20/40. Corneal topography revealed simulated keratometric readings of OD 41.12 @ 125/47.12 @ 035 with 5.87D of corneal astigmatism and OS 43.00 @ 035/43.50 @ 125 with 0.50D of corneal astigmatism (Figure 2).
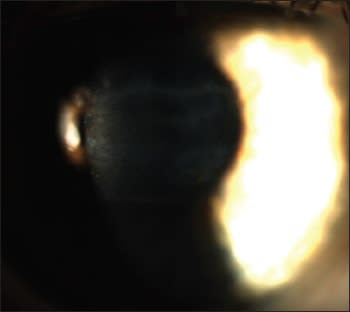
Figure 1. Patient's post-HSV scar.
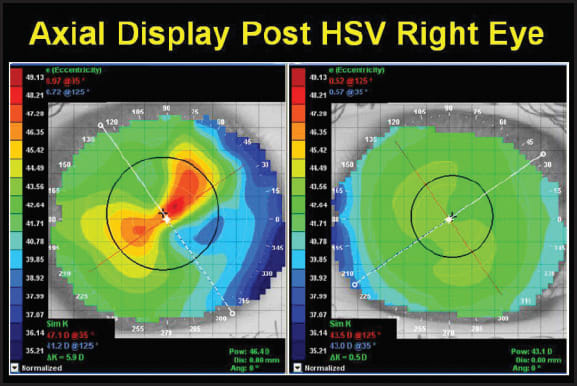
Figure 2. Post-HSV corneal topography.
Which Topography Map to Use
Figure 3 shows the axial and elevation maps of the patient's right eye. It is clear that the elevation map provides a more accurate description of the corneal shape as evidenced by the final fluorescein pattern. The patient was fitted with a bitoric GP lens OD that produced a final VA of 20/25+1.
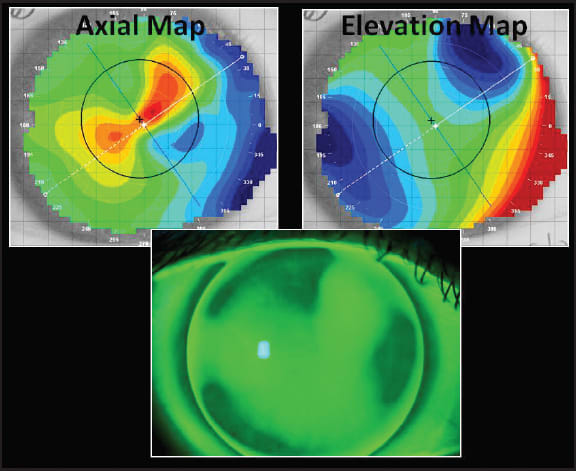
Figure 3. Axial map, elevation map, and fluorescein pattern of the patient's right eye.
When viewing corneal topography maps, the axial display map provides the most accurate description of corneal power and corneal toricity; however, it does not indicate how high or low the geographic spots are on the corneal surface. Axial maps are, in fact, somewhat counterintuitive in that you naturally acquaint the color red of the axial map with the “highest” spot on the cornea, and this is not always the case.
The elevation display best describes the actual shape/height of the cornea. With this display the highest portions of the cornea are red while the lowest are blue, a complete opposite of the color code used in the axial maps.
This feature of the elevation display can be best illustrated by viewing the fluorescein pattern of the GP lens on-eye. Here, it is easy to see that the lens is in closest proximity to the cornea where the cornea is the highest (red/green in the elevation display and blue in the axial display). The lens clears the cornea across the portions that are lowest (blue/green in the elevation display and red in the axial display). The height feature of the elevation display is what allows modern corneal topography systems to create simulated fluorescein patterns with great accuracy. CLS
Patrick Caroline is an associate professor of optometry at Pacific University. He is also a consultant to Paragon Vision Sciences. Mark André is an associate professor of optometry at Pacific University. He is also a consultant for CooperVision.