


GP Insights
Strategies for Decreasing the Impact of Scleral Lens Debris

By Gregory W. DeNaeyer, OD, FAAO
One of the most common complications of scleral lens wear is the slow buildup of debris in the fluid reservoir between the lens and the cornea during the course of a day (Figure 1). The debris can consist of mucin, mucus, epithelial cells, meibum, or makeup. Reservoir debris is more of a problem with scleral lenses that are 18mm or larger because they hold larger reservoirs and have slower fluid turnover. Mucus buildup can be considerable in patients who have severe ocular surface disease (Figure 2).
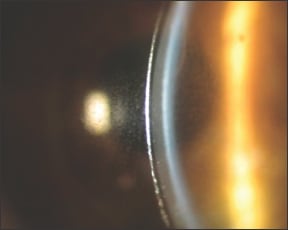
Figure 1. Buildup of debris between lens and cornea.

Figure 2. Mucus buildup in a patient with ocular surface disease.
For the most part, as long as there is continuous turnover of the fluid, then reservoir debris usually will not negatively affect the anterior ocular surface. However, stagnation of this debris, as in the case of a sealed lens that is preventing fluid exchange, can result in a “toxic swamp” that leads to an inflammatory cascade (Breece, 2009). Loosening the peripheral curves to return the lens to a semi-sealed, fluid-exchanging state will resolve this complication.
More commonly, significant debris accumulation will cause some patients to complain of foggy vision that is not attributable to poor surface wetting. A patient's individual visual sensitivity to debris can vary considerably. The following strategies may be helpful for patients who are visually symptomatic to debris.
Patient Strategies
1. Instruct patients to remove the lens, rinse it, and refill it during a mid-day break. Informing patients that this may be necessary during the fitting process will help ensure better acceptance of such breaks once they start wearing the lenses. Patients who have dry eye tend to experience more debris and are more likely to require rinse and refill sessions (Visser, 2007).
2. Have patients use a more viscous solution to fill their contact lens before application. One option is the off-label use of non-preserved carboxymethylcellulose, which may increase the time for debris to make its way beneath the lens.
3. Lower the vault of the contact lens so that there is effectively less reservoir and therefore patients won't have to look through as much debris.
4. Refit patients into smaller-diameter lenses that hold less reservoir and have more efficient tear exchange.
5. Off-label use of topically prepared 10% Mucomyst (acetylcysteine, Bristol-Myers Squibb and generics) can be prescribed one to two times per day. This mucolytic agent, which is normally used for bronchiopulmonary disease, can dramatically reduce mucus accumulation.
Keep in mind that if you notice significant debris beneath the lens but the patient is not complaining and the cornea is healthy, then no additional action is necessary. CLS
To obtain references for this article, please visit http://www.clspectrum.com/references.asp and click on document #184.
Dr. DeNaeyer is the clinical director for Arena Eye Surgeons in Columbus, Ohio. His primary interests include specialty contact lenses. He is also a consultant to Visionary Optics. Contact him at gdenaeyer@arenaeyesurgeons.com.