


OCULAR ALLERGY
Managing Allergy in Contact Lens Wearers
A thorough evaluation, proper diagnosis, and timely treatment will help you bring relief to allergy sufferers.
By Jeffrey Krohn, OD, FAAO, & Alesha Jensen, OD
We have been hearing for years that ocular allergy sufferers are frequent, but symptoms are often under-reported and therefore under-treated. While it would seem natural for practitioners to increase their efforts in properly caring for these patients, there is still a disconnect. Many patients assume that they have to “live with allergies,” and they either don't think to ask for treatment or they go looking for “self-treatment” options. They will be grateful and loyal to the practitioners who bring them relief.
It sometimes seems that modern eye care has either a stalwart dedication to basic refractive care or an enthusiasm to provide care for extreme medical conditions only (e.g. glaucoma, age-related macular degeneration, etc). The conditions that become everyday annoyances to patients often go unaddressed. It is our responsibility as eyecare practitioners to resist focusing on these two extremes, to ask about symptoms of discomfort, to perform a complete anterior segment evaluation, and to treat our patients' underlying problems.
Prevalence of Ocular Allergy
According to the American Academy of Asthma Allergy and Immunology (AAAAI), one in five people have allergies with ocular involvement. It was estimated in 2003 that the United States had more than 30 million contact lens wearers. The combination of ocular allergies and contact lens wear can lead to discomfort, creating a trend of increasing numbers of contact lens wearers becoming part-time wearers or discontinuing wear altogether. According to Prescription Audit (by Scott-Levin, Inc.) in 2000, 41 million over-the-counter ocular allergy medications were sold compared to the four million prescription ocular allergy medications filled. This indicates that there is a large population of allergy suffers who could benefit from newer and better methods of treatment.
If the majority of these individuals are “self-treating,” as is commonly thought, the tendency of patients to keep symptoms to themselves should be a wake-up call. We need to diligently ask about symptoms, evaluate meticulously for clinical signs, and initiate therapy to make contact lens wear as comfortable as possible to prevent dropouts. Appropriate history, diagnosis, and treatment are essential for successful contact lens wear in this population of patients.
Diagnosing Allergy
Accurate diagnosis of ocular allergies begins with the case history. Prudent practitioners will ask about general symptoms of ocular discomfort. The answers are not likely to lock them into a particular diagnosis, but will demonstrate that there is discomfort that needs relief. A general question to each patient asking them whether they experience “any burning, stinging, itching, or dryness” will provide an adequate “net” with which to catch those suffering from lid disease, tear film dysfunction, allergies, contact lens intolerance, or some combination of these.
Next, it would be appropriate to determine acute versus chronic conditions, so establishing a timeline of the symptoms is appropriate. Most practitioners are familiar with the appearance, symptomatology, and appropriate treatment of an acute allergic or infectious response to an exogenous stimulus. What deserves more attention is the differentiation of symptoms related to lid disease, tear film dysfunction, and chronic/seasonal ocular allergies.
Remember that toxins, desiccation, and the allergic cascade will all be exacerbated by contact lens wear and will be reported by affected patients using similar vernacular. Nevertheless, a symptom of “itching” should make you consider a working diagnosis of either lid disease (blepharitis or meibomian gland dysfunction) or allergies. Asking whether the itching seems to originate from the “skin of the eyelid” versus the eye itself can be of great utility.
We have found that with symptoms of “burning,” “dryness,” or “stinging,” it is most helpful to ascertain when the symptom occurs. Details that corroborate the symptom with time of day, duration of lens wear, or extraneous irritants (ceiling fans, driving, wind, animals, etc.) can be invaluable. A history of previous “styes” by the patient would also have enormous significance.
While “discharge” may lead us toward infectious etiology, “tearing” or “watering” deserves strong consideration as being allergic in nature. Whether the watering comes from the eye nasally (over-production) or temporally (poor lid function) can be helpful.
The contact lens history deserves a notable amount of effort as well. Note any tendency for overwear or under-cleaning, as well as use of “old-generation” multiple purpose solutions (i.e., generic).
Objective assessment begins with external observation. Any erythema, swelling, or “weeping” appearance to the eyelids, along with “pointing” of the lashes, would be significant, as would a gross observation of the amount of ocular redness and its asymmetry.
Biomicroscopic evaluation begins with the eyelid skin, lids, and lashes. Devote particular attention to the quality and quantity of the lacrimal lake along the lid margin as well as to the patency of the meibomian gland orifices. This last observation, along with digital expression of the glands and evaluation of the expressed contents, is perhaps the most often overlooked test in evaluating patients who have ocular discomfort.
The use of both fluorescein and lissamine green to evaluate the cornea, conjunctiva, and tear film have been well described and should not be omitted from the workup. Particularly, the presence of any corneal staining will move you away from an allergic diagnosis and toward either lid or tear dysfunction; ocular allergic response rarely demonstrates staining. Evaluation of the conjunctival responses, both bulbar and palpebral, will usually demonstrate either a notable response (in the acute/toxic presentations) or minimal response (in chronic cases). Most clinicians are familiar with papillary versus follicular reaction and the need for eversion to evaluate for mechanical/toxic giant papillae, and it is hoped that all contact lens practitioners are evaluating the superior tarsal plate regularly when examining contact lens patients. Of particular interest is the “heaviness” or “redundancy” of the bulbar conjunctiva. It may take a practitioner some time to become familiar with normal bulbar conjunctival “tension” and to properly identify edema (chemosis) and redundancy (conjunctival chalasis). This latter condition is of particular interest in the elderly population and, in our opinion, is often the cause for temporal epiphora.
We believe, therefore, that diagnosing ocular allergy as the cause for non-acute ocular irritation is somewhat of a diagnosis of exclusion, or more often, a diagnosis that coexists with lid disease, tear dysfunction, and/or environmental toxins. While this will be addressed when we discuss management, one additional issue is relevant to diagnosis. As eyecare practitioners, many of our patients see us once a year. Given that the timing of their examination may or may not occur at the time of seasonal allergic symptoms, many of our patients will be free of all clinical signs and symptoms of the allergy process. Patients who presents with a “white and quiet” eye may therefore still need special attention and instruction.
Managing Ocular Allergies
Given this perspective of ocular discomfort, management becomes a creative “concoction” of various approaches to the differing components relevant to the individual presentation. Patients may leave with instructions, prescriptions, and/or accoutrements useful for any of the above mentioned conditions. Here we will present our perspective on these management strategies in clinical care.
Compresses Cold compresses can be very helpful for a very itchy and irritated eyelid/adnexa. Various home remedies abound (ice chips, frozen vegetables, etc), as well as gel masks and goggles.
Heated compresses are recommended for meibomian gland irregularities. While home remedies have been suggested, we find them messy and adherence poor. We recently began using goggle-type units with reusable inserts. For regular nightly hygiene, inexpensive hand-warmers (www.snapheat.com) are wonderful tools. The trick is to provide heat in both the proper temperature and duration.
Hygiene You should consistently instruct your patients who experience ocular irritation about eyelid cleansing, utilizing a commercially prepared product for that purpose. To allow mild-to-moderate presentation of lid disease to go untreated and then suddenly become attentive when the lids are markedly indurated, erythematous, and painful is inexcusable. Most patients who have ocular irritation will benefit from regular cleansing. It has been our observation that men typically need this attention more than women do, presumably because men do not perform nightly eyelid makeup removal and they have concerns about “getting soap in the eyes.” It should be our message that a little soap around the eyes is a good idea.
Lubrication While the choice of an appropriate ocular lubricant is not the focus of this article, it is worthwhile to educate yourself in the delicate differences among formulations. We have found that most patients are most successful with an emulsion that attempts to mimic the lipid layer such as Systane Balance (Alcon) or Soothe XP (Bausch + Lomb).
Hyperosmotic While salt-based ointments were our only option up until a few years ago, we have found new life for the use of hyperosmotic therapy with the introduction of FreshKote (Focus Laboratories). This novel medication provides wonderful relief for patients who have an irregular, poorly healing corneal epithelium. Patients who benefit from it most usually have concurrent lid disease and are also treated with an antibiotic with anti-inflammatory activities. FreshKote is a “behind the counter” medication that does require a prescription. We utilize it to promote corneal healing and then taper the medication once healed.
Antibiotics The use of both Azasite (Inspire Pharmaceuticals) and Doxycycline for treating lid disease has been discussed extensively. Azasite works well as a topical lid medication; we have patients rub the drop into the lower lid and then rest with the eyes closed for two to three minutes. Using an oral medication has risks and benefits that should be considered carefully. Two unique formulations of Doxycycline that we believe are well suited to lid disease management are Oracea and Periostat. The first is a 40mg capsule with 30mg of immediate activity and 10mg of delayed-release granules. The second is a lower dose (20mg) that can be more easily tolerated in individuals who have experienced difficulty resulting from a reduction in normal bacterial flora, either intestinal or vaginal.
Contact Lens Modification Treat contact lens patients on an individual basis depending on their contact lens material, replacement schedule, and care system used. Reducing wear time can often help alleviate acute symptoms, and increasing replacement frequency can be beneficial as well. Heys et al (2003) showed that switching ocular allergy sufferers to daily disposable lenses improved comfort for 67 percent of wearers compared to only 18 percent improved comfort in those who simply replaced their reusable lenses. This demonstrates the importance of increasing replacement frequency in lens wearers who suffer from ocular allergies.
In cases in which this modality is not feasible, it is important to emphasize the importance of the care system. Peroxide-based systems (e.g. Clear Care [Ciba Vision]) can be used as an alternative to multi-purpose solutions. Avoid extended wear in patients with anything less than a “pristine” ocular surface.
Oral Antihistamines Patients suffering from ocular allergies also often have systemic allergy symptoms. Therefore, it is common that such patients are taking systemic allergy medications. These systemic allergy medications, both over-the-counter and prescription, can increase dryness of the ocular surface. Topical agents deliver high concentration of medication to the ocular surface with fewer side effects compared to oral medications.
Topical Antihistamines Topical antihistamines compete with histamine at the receptor sites, providing short-duration relief of itching. Mast cell stabilizers are preferred; their method of action is to prevent histamine release from the mast cell. The drawback to mast cell stabilizers is the long onset of approximately 10 to 14 days before relief occurs. Therefore, the most common treatment for ocular allergies is an antihistamine and mast cell stabilizer combination, which helps with both the acute itchiness and the long-term treatment of stabilizing the mast cell. This medication is most effective when used on a consistent basis and dosed prior to the onset of the allergy season.
This brings us back to patients who present for examination at a time different from their allergy “flare-ups.” Make some arrangement with these patients to provide access to care during their time of discomfort.
Topical Anti-Inflammatories Non-steroidal anti-inflammatory drugs (NSAIDs) are approved for use with ocular allergic symptoms (usually itching) and are desirable by most clinicians and patients. Topical corticosteroids can successfully reduce ocular inflammation, but should be reserved for cases that are acute or moderate-to-severe in intensity or in cases of atopic, vernal, and contact lens papillary conjunctivitis. Corticosteroids are not a good long-term treatment option as the ocular side effects of prolonged use include increased intraocular pressure and risk of cataract formation. Newer “soft” steroids appear to have a much safer profile for patients who require prolonged therapy.
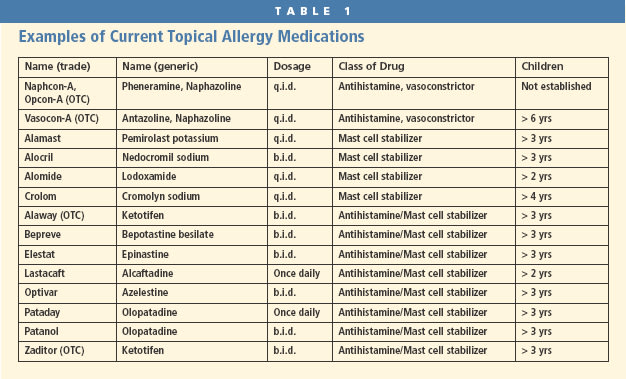
Contact Lens Wear and Medications Advise contact lens wearers to use topical medications approximately five to 10 minutes prior to contact lens application. No drops should be used during contact lens wear. A once-daily dosing of an antihistamine/mast-cell stabilizer such as Pataday (Alcon) works well with contact lens wearers, as they can dose in the morning prior to application, and allergic relief should last all day. Other twice-a-day dosing combinations can also be useful when dosed before lens application and upon contact lens removal at the end of the day. Table 1 lists most topical ocular allergy medications.
Summary
As mentioned previously, symptoms of ocular irritation are under-reported by patients. Therefore, it is up to us to initiate a conversation about ocular discomfort with all patients, especially those wearing contact lenses. Thorough evaluation, proper diagnosis, and timely treatment are essential in the success of our allergy sufferers who wear contact lenses. CLS

| Dr. Krohn is in private practice in Fresno, Calif. He is a Diplomate in the Academy of Optometry Section on Cornea, Contact Lenses and Refractive Technology. He is also a Vision Source doctor and administrator and a clinical investigator for Vistakon. |

| Dr. Jensen is a graduate of Southern California College of Optometry and is a Vision Source doctor. She is in private practice in Fresno and Hanford, Calif. |