


KERATOCONUS FITTING
Evaluating Virtual Fitting for Keratoconus
This study set out to determine how accurately a topographer's software could predict fluorescein patterns when fitting contact lenses for keratoconus.
By Christine W. Sindt, OD, FAAO; Trudy K. Grout, FCLSA, NCLC-AC; & Randy Kojima, FAAO, FOAA
Keratoconus is a common corneal ectasia that frequently frustrates both patients and practitioners. Many fitters lack the experience or the resources to justify large fitting sets. Even in practices with many keratoconus patients and ample fitting sets, the chair time involved with placing multiple lenses on the eye is laborious and expensive. From the patients' perspective, multiple trips to their practitioner, only to discover that yet another lens needs to be ordered, has an economic impact of missed work and direct out-of-pocket expenses. There is a mental impact of a laborious fit on patients as well, including disappointment, anger, and eventual loss of confidence in the practitioner. All too often, the practitioners pay the cost of the multiple remakes and lost chair time.
Unfortunately, many practitioners have decided that the costs associated with fitting keratoconus patients are just too high, and they refrain from future fits, sending patients out of the practice and often hundreds of miles away to a “keratoconus doctor” for contact lens fitting or surgery.
To overcome the problems of fitting sets and chair time, it would be beneficial if we could do “virtual fitting” using topography and virtual contact lens fitting sets.
Are Topographers Accurate Enough?
When considering employing corneal topographers for contact lens design, we must ask: are they accurate enough? The majority of topography instruments in clinical practice are based on placido disk technology, which captures its information (shape and elevation) by reflecting rings off the cornea surface. A smooth, even tear film, devoid of tear breakup, is critical for accurate corneal shape and elevation determination. Without quality ring reflection, the corneal topographer cannot accurately calculate the shape of the eye.
If the instrument is able to reflect the rings, then the topographer can interpret the corneal surface a number of different ways. Axial and tangential interpretations are used to describe corneal shape and can be applied in our determination of the initial lens parameters. Another important interpretation is the elevation map, which can predict areas of lens bearing and clearance. However, the above functions do not predict the actual fluorescein pattern that a lens would have on the eye. In other words, if the ultimate goal is to fit the patient with a GP lens, what would a specific lens look like on-eye? What should be the ideal base curve or diameter? What optical zone is most appropriate? Will there be areas of excessive bearing or lift that should be accounted for? Should a toric or asymmetrical lens design be considered? There are many questions that an accurate interpretation of fluorescein pattern could answer without placing a lens on-eye, waiting for settling, then spending chair time for evaluation.
In our study, we employed the Medmont E300 corneal topographer (Precision Technology), which uses an arc-step algorithm to build the shape and elevation of the eye from each of the 32 reflected rings using approximately 15,000 data points. We evaluated the instrument's ability to effectively construct the elevation of the cornea and virtual GP fluorescein pattern and compared this to the actual fluorescein patterns of keratoconus patients fit with identical lenses.
Methods
In accordance with the University of Iowa Institutional Review Board, keratoconus patients were identified during regularly scheduled clinic appointments at the University of Iowa Department of Ophthalmology and Visual Sciences. Patients who had keratoconus or pellucid marginal degeneration, were older than 18 years of age, and who had not had any ocular surgery or other concomitant disease were invited to participate in the study. Study subjects did not receive compensation for participation. Patient data was stored in compliance with the Federal Health Insurance and Portability and Accountability Act.
Once informed consent was obtained, we performed corneal topography using the Medmont E300. Care was taken to image with the largest fissure size, maximum ring reflections, and image centration on the cornea. We performed several scans to assure overall map quality and reproducibility.
Two keratoconus lens designs were installed in the Medmont contact lens fitting program: the Keratoconus Bi-Aspheric or KBA (Essilor Contact Lens and Precision Technology) and the Rose K2 (Menicon/Blanchard Contact Lens and distributors).
After choosing the best topographic image, we chose the parameters of a theoretical lens using the Medmont software in concordance with the available fitting set base curves and diameters. The lenses were designed to have a minimum of 20 microns of apical clearance with definite vaulting over the cone if possible.
As an example, Figure 1 shows an image of the Medmont E300 contact lens module showing the theoretical fluorescein pattern of a keratoconus lens (KBA) on a patient who has oval keratoconus. The white line running vertically across the theoretical fluorescein pattern indicates the axis of the tear layer thickness on the graph below. Various tear layer thicknesses in microns are displayed along that axis line using arrows pointing to the same spot on the graph.
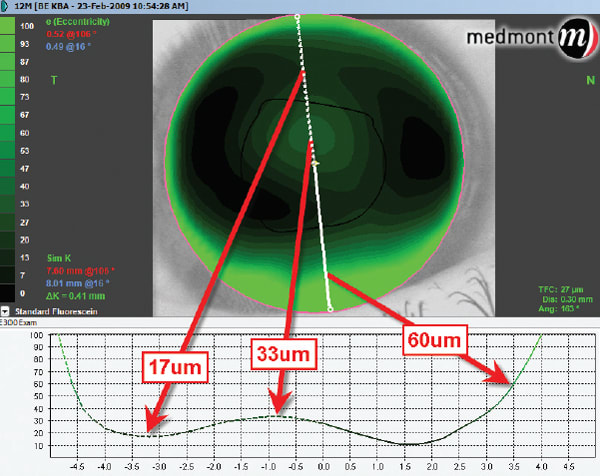
Figure 1: Image of the Medmont E300 contact lens module showing the theoretical fluorescein pattern of a keratoconus lens (KBA) on a patient who has oval keratoconus.
In each case, the same lens as the theoretical lens was placed on the eye and the fluorescein pattern was photographed using an INOVA 5 LED cobalt flashlight, Tiffen yellow filter, and Canon 780IS camera.
We analyzed both theoretical and actual fluorescein patterns for pattern similarities. Patient-related factors such as comfort and visual acuities were not assessed.
Results
Thirty-one lens fits of 18 subjects were analyzed. Table 1 summarizes the 31 fits. Of the 18 subjects, we evaluated the topographies of 29 eyes. Twenty-one topographies had good ring quality, while 10 topographies were considered poor quality. We defined good ring quality as parallel ring reflection with an absence of tear film breakup or scar-induced distortion of the placido rings. Poor quality images were those with distortion of the placido reflection causing two or more rings to collapse or touch each other (absence of parallel ring reflection).
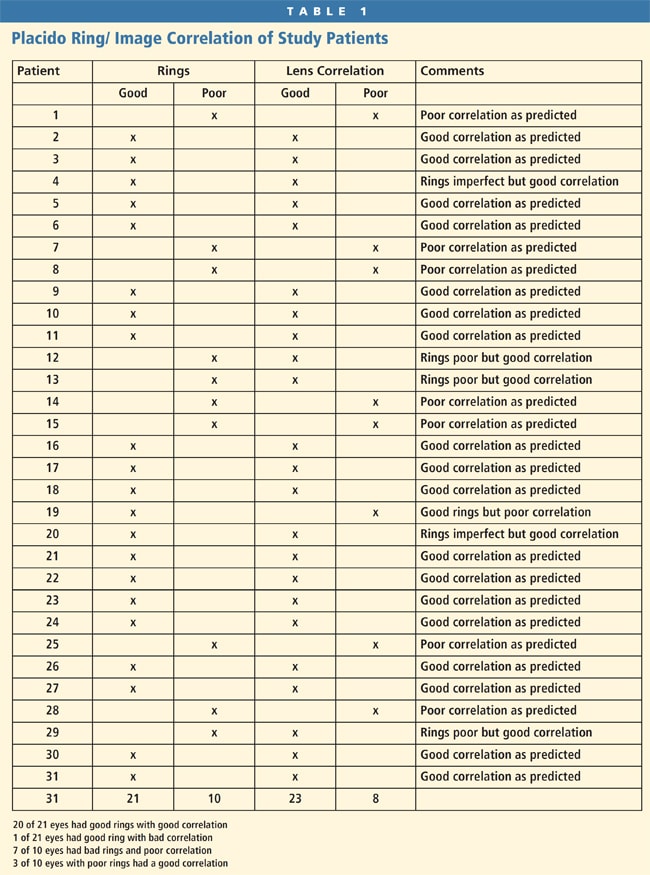
Theoretical fluorescein patterns were correlated to actual fluorescein patterns in 31 fits. Two eyes had both types of contact lens designs fit on the same eye. In 23 of 31 eyes (74 percent), a good match of theoretical to actual fluorescein pattern was found. In comparing the two images, the accuracy or agreement in apical clearance was evaluated as well as points of bearing and areas of fluorescein thinning and thickening. Any lid interaction causing tilt on-eye was taken into account when evaluating the actual pattern as compared to the software's prediction, which doesn't model such forces. The theoretical and actual fluorescein patterns were well correlated (Figure 2) when the placido rings demonstrated parallel and even ring reflection. This is logical because to build the corneal elevation properly, placido disk topographers must achieve a quality reflection off the corneal surface (free of tear breakup or scar-induced ring distortion). When evaluating our outcomes based on the number of topographies that had quality photokeratoscope images, 20 of 21 eyes showed an excellent correlation of theoretical and actual patterns. When calculating diagnostic lenses based on a quality ring reflection, the topographer was able to accurately predict the fit in 95 percent of the cases.
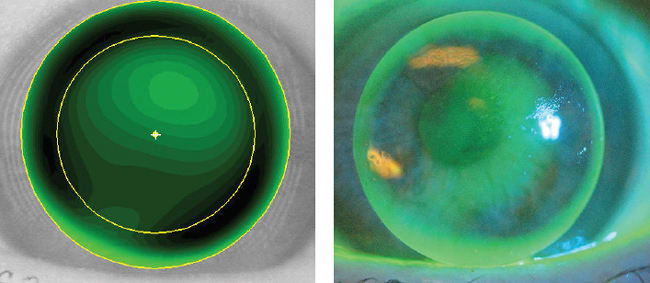
Figure 2. The Medmont topographer's contact lens module is used to build an initial Rose K2 trial lens for this eye. The second image shows a diagnostic lens with the same parameters on-eye.
As an example, Figure 3 shows an initial KBA trial lens selected from the Medmont topographer's contact lens software. Note the similarity in the pattern when the same trial parameters were placed on-eye. With a quality reflection of the placido rings off the corneal surface (Figure 4), the topographer is able to accurately construct the shape and elevation of the cornea. The contact lens module can then accurately predict the pattern of the GP lens with a high correlation of theoretical to actual.
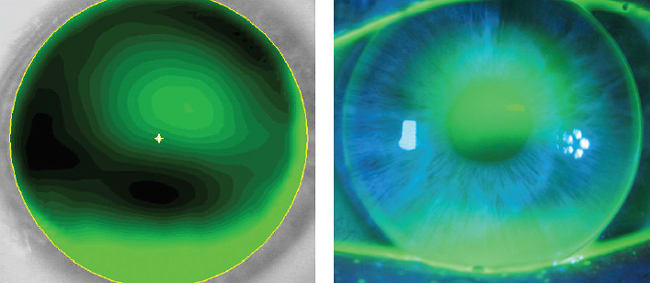
Figure 3. Predicted KBA diagnostic lens versus actual KBA lens with same parameters of 7.10mm base curve, 10.2mm diameter, 0.98 eccentricity on-eye, showing good correlation.
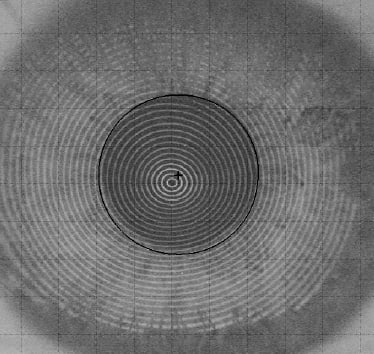
Figure 4. Photo keratoscope image of the placido rings reflected off the corneal surface of the patient from Figure 3. Note the parallel and even ring reflection that results with the absence of tear breakup and a cornea free of scarring or imperfections in the epithelial surface.
In 8 of 31 cases (26 percent), no correlation or a very poor match could be found in comparing the topography-generated fluorescein pattern and the actual diagnostic lens fluorescein pattern on-eye (Figure 5). The contact lens module's predicted pattern in Figure 5 does not correlate with the same trial parameters on-eye. In this case, the patient's corneal scarring caused significant distortions in the placido rings (Figure 6), which hindered the topographer's ability to build the sagittal depth of the eye. The error in building the shape and elevation of the cornea resulted in contact lens module error and a poor correlation of the predicted and actual lenses. In 7 of 8 eyes (88 percent), this poor correlation could be attributed to obvious distortion in the placido disk rings, which is apparent in the case of one patient who had one eye with scarring and one eye without (Figures 7 and 8). As mentioned earlier, tear breakup and scarring can impede quality light reflection off the cornea. Distortions in the placido rings hinder accurate calculation of the eye's elevation, which results in contact lens module error.
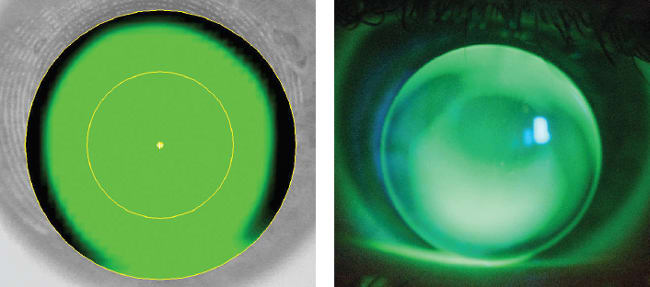
Figure 5. Predicted Rose K2 parameters versus actual lens on-eye, showing poor correlation.
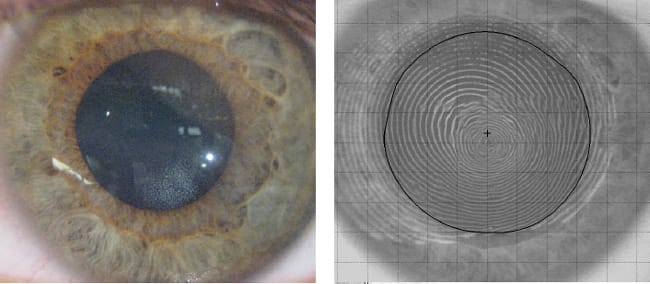
Figure 6. Same patient as Figure 5. This patient's corneal scarring resulted in poor quality ring reflection that ultimately caused the poor correlation between the predicted and actual fluorescein patterns.

Figure 7. A right eye with the parameters of the theoretical Rose K2 GP designed (left) and actual diagnostic lens with the same parameters (right). Note a poor correlation between the two on this patient. The placido displayed severe ring distortion from the patient's heavy central scarring, which hindered the accuracy of the contact lens module.
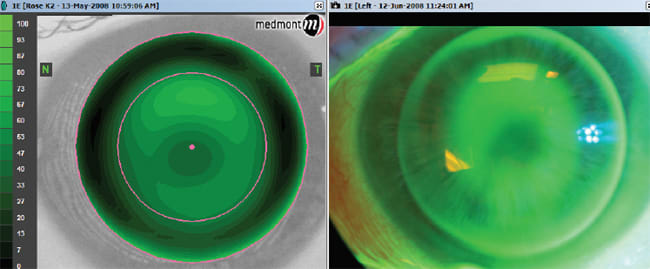
Figure 8. The same patient as in Figure 7 showing the left eye with good correlation between the theoretical Rose K2 lens (left) and the actual diagnostic lens of the same parameters (right).
The topographer could not predict the correct fluorescein pattern in 1 of 22 eyes when the placido rings were ideal. However, it was interesting that in 3 of 10 cases when the photokeratoscope image showed ring distortion from corneal scarring or severe dryness and “ring jam,” the topography software was able to predict the correct fluorescein pattern.
Conclusion
It is clear from this study that the Medmont corneal topographer can be used to design the initial GP lenses even for patients who have diseased eyes such as keratoconus and pellucid marginal degeneration. But it is equally apparent that the accuracy of the topographer's contact lens fitting module is hindered by distortions in the placido rings (tear breakup and corneal scarring). To use this tool effectively for custom or diagnostic lens selection, practitioners must ensure that the placido rings are reflected in a parallel and even manner back to the instrument.
Moving forward, it is imperative that GP manufacturers include their designs in the contact lens modules. The economics of patient chair time, both for patient and practitioner, as well as the wide availability of corneal topographers will insure that this will be a must-have technology of the future to improve our GP contact lens fitting efficiency on diseased eyes. CLS
The authors would like to thank Medmont for loaning the University of Iowa the equipment used for the duration of the study.
| Dr. Sindt is a clinical associate professor of ophthalmology and director of the contact lens service at the University of Iowa Department of Ophthalmology and Visual Sciences. She is also the 2010-2011 Chair of the AOA Cornea and Contact Lens Council. She is a consultant or advisor to Alcon, Ciba Vision, and Vistakon and has received research funds from Alcon. You can reach her at christine-sindt@uiowa.edu. |
| Trudy Grout works in the Department of Ophthalmology and Visual Science, University of Iowa Health Care in the Contact Lens Clinic. She currently is a member of the CLSA Fellowship Committee. She has received research funding from Alcon. |
| Randy Kojima is director of Technical Affairs for Precision Technology in Vancouver, B.C. and also serves as research scientist and clinical instructor for the Pacific University College of Optometry in Forest Grove, Ore. |