


GP Insights
Fitting a Rigid Prosthetic Lens

By Gregory W. DeNaeyer, OD, FAAO
Utilizing contact lenses for cosmetic anterior segment restoration is an important niche of a specialty contact lens practice. Soft contact lenses are often used and can be manufactured as computer-generated prints or hand-painted prosthetics. Generally, soft lenses are able to provide most patients with a successful means to regain normal ocular appearance after disease or trauma has resulted in significant corneal opacity.
However, severe irregularity or a scleral obstacle can result in an ill-fitting soft lens that diminishes the desired cosmetic result. In these cases, rigid corneal or scleral lenses may be a better option. Unfortunately, the properties of GP materials make them difficult to paint, and so PMMA is most commonly used. Obviously, the challenge of using PMMA material is the possibility of hypoxia-related complications because it is not permeable to oxygen. This is especially a concern with a scleral-type lens that has extremely slow tear exchange.
A Case in Point
A 25-year-old female patient who had a scarred and blind left eye secondary to proliferative diabetic retinopathy, retinal detachment, and glaucoma (Figure 1) reported for a prosthetic lens evaluation. Examination revealed only a mildly irregular corneal surface, which a soft lens could easily drape, but she had a sizeable conjunctival bleb at the 12 o'clock position from a previous trabeculectomy. She also had mild exotropia that resulted from loss of binocular fusion. The concern with using a soft lens was that the bleb would push the lens excessively down, making it difficult to keep a painted soft prosthetic lens in its ideal position.
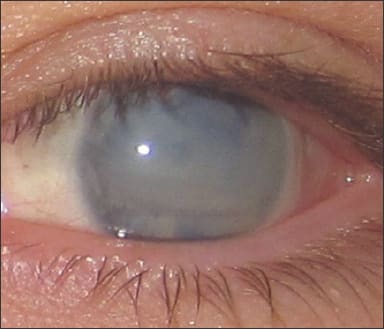
Figure 1. Patient's complete corneal opacification and exotropia.
We decided to trial a PMMA lens with a beveled notch to accommodate the bleb, and if successful, a prosthetic version could be manufactured for the patient. After fitting the lens and before painting, the patient wore the lens on a daily wear basis to test tolerance and hypoxic sensitivity. At the end of the trial, the patient reported wearing the lens comfortably, and no corneal neovascularization, edema, or bleb injury was present. The lens was dotted slightly nasal of center to indicate the amount of offset that was needed for the lens to mask the patient's exotropia.
A digital photograph, along with photopic pupil size and horizontal visible iris diameter of her right eye, were sent with the lens to Cantor + Nissel for manufacturing the prosthetic version. The process involved first producing a PMMA mold of the lens that had been successfully fit. The molded lens was cut back, painted, and resealed with PMMA. The finished lens matched the patient's normal right eye perfectly (Figure 2) and offset her exotropia so that her eyes looked naturally aligned. The patient was thrilled with the results.

Figure 2. Prosthetic scleral lens that includes a painted haptic and beveled notch.
A Rewarding Skill
Using rigid lenses for cosmetic restoration can be every bit as rewarding as using them to improve vision by masking corneal irregularity. CLS
Dr. DeNaeyer is the clinical director for Arena Eye Surgeons in Columbus, Ohio. His primary interests include specialty contact lenses. He is also a consultant to Visionary Optics. Contact him at gdenaeyer@arenaeyesurgeons.com.