


KERATOCONUS
Fitting Keratoconus After Intracorneal Ring Implants
Improved visual acuity can be achieved with a GP lens specifically designed for these challenging corneas.
By Luciano Bastos
I believe that intracorneal ring implants can benefit patients who have mild-to-moderate corneal ectasia by improving their visual acuity with or without additional correction. It is also thought that the main objective of this procedure is to prevent keratoconus progression. In many cases, however, visual acuity after the procedure is not good enough to help patients even when corrected with eyeglasses. These patients may still need contact lens correction to achieve optimal visual acuity.
It is important to mention that contact lens intolerance in patients who have keratoconus is generally due to an improper lens design or technology or an improper fitting strategy. Therefore, it is of utmost importance to prescribe high-quality specialty GP designs when fitting keratoconus to achieve the best results, patient compliance and fitting success.
Complex Fitting Challenge
Fitting contact lenses to keratoconus patients can be difficult, depending on a patient's specific corneal characteristics. Fitting keratoconus after intracorneal ring implantation may be one of the most challenging situations, even when the keratoconus is not advanced. The complexity of the fitting is due to the presence of the abnormal elevation in the inferior paracentral area of the cornea. The inferior part of one of the ring segments is usually located in a thinner region of the cornea, causing an anterior elevation in this area that, in turn, affects the fitting. Most GP contact lenses will not vault this area of the cornea, which can lead to keratitis and localized corneal erosion.
In Brazil where my practice is located, we frequently see keratoconus patients who have developed GP lens intolerance after intracorneal ring implantation, and we understand this is caused by the paracentral elevation. To resolve this problem, most practitioners in Brazil tend to fit specialty soft keratoconus lenses or a piggyback system to preserve visual acuity and corneal health. One problem we must consider when fitting soft silicone hydrogels, frequent replacement hydrogels or piggyback lens systems is that keratoconus patients frequently have abnormal tear film stability. This is also frequently associated with corneal hypoxia and conjunctival hyperemia. If a patient works or lives in an air-conditioned environment, the symptoms may appear earlier or be more severe.
Following are some challenging cases in which we were able to successfully fit a GP lens over the elevation in keratoconus patients who had undergone intracorneal segment implants.
Case 1: Customized Solution
This 24-year-old man had moderate bilateral keratoconus with intracorneal implants in the left eye. He presented with an extrusion of the nasal segment, and he had only the temporal segment (Figure 1). The patient had been fitted with several brands of GP lenses for keratoconus, but he developed lens intolerance. He was then fitted with a piggyback system, but in less than 6 months, he showed signs of conjunctival hyperemia and corneal hypoxia.

Figure 1. Note the elevation around the inferior extremity of the temporal segment; the photo is turned to the right for better visualization.
We initially fit the right eye with a GP Ultracone lens (Ultra-lentes, Brazil) designed for keratoconus. We observed that with this lens design, the elevation caused by the inferior extremity of the corneal ring was high enough that the lens would bear on it and cause corneal staining. To address this, we developed a customized solution using the Ultracone Post-Corneal Ring (PCR) GP lens, also manufactured by Ultralentes. We increased the back optical zone and the sagittal depth so the lens would vault the entire central and paracentral cornea without touch while preventing air bubbles (Figure 2). This multiaspheric design was comfortable enough to help the patient adhere to the adaptation process and succeed with his new lens. Figure 3 shows this patient after 3 months of wearing this lens all day and removing it only to sleep.
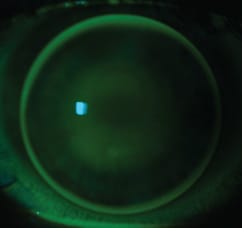
Figure 2a. Ultracone PCR Customized fitting.
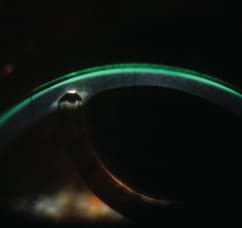
Figure 2b. Tear film flowing free, no touch.
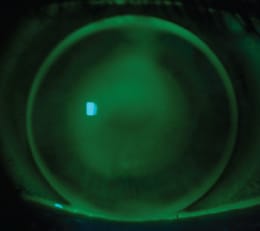
Figure 3. Overall view of the Ultracone PCR fit.
Case 2: Improved Vision and Lens Tolerance
This 23-year-old woman with bilateral keratoconus had intracorneal ring implants in both eyes. She complained of poor vision, contact lens intolerance and many prior GP lens fittings with different specialists. Her best-corrected visual acuity with spectacles was 20/40. She was disappointed that she did not have better quality vision. Figure 4 shows the anterior segment upon evaluation.

Figure 4. Intracorneal ring segments very close to each other at 8 o'clock.
In this case, the corneal ring segments together formed a higher elevation pattern along the tunnel ducts, but they were positioned close to each other so it was possible to achieve a good fitting relationship. We fitted an Ultracone PCR GP lens. We modified the second zone to maintain the lens positioned superi-orly where the best lens-to-cornea fitting relationship was achieved. If we fit a lens with the standard secondary aspheric curve, it tended to drop (Figure 5a). Comfort was achieved, corneal physiological health was maintained, and final visual acuity was 20/20 (Figure 5b).

Figure 5a. Initial test with Ultracone PCR (OD).
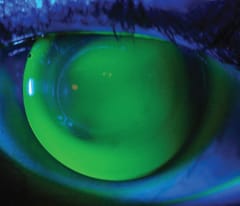
Figure 5b. Ultracone PCR custom modified (OD).
Achieving the Best Fit
These cases demonstrate that improved visual acuity can be achieved after intracorneal ring implantation. The use of anterior elevation data helps us understand the unique corneal topography created by the implants, and the use of high-quality, high-performance specialty GP diagnostic lenses leads to the best possible solution for each patient.
Although we have very good contact lens software programs, sometimes they cannot accurately estimate the entire shape of these irregular corneas. In addition, other factors must be evaluated, such as tear film, dioptric maps, corneal biomechanical resistance and lid apertures, as well as the contact lens quality, design and technology. To address complex corneal irregularities and problem-solve for our patients, we need to consider all of these factors and use all available resources. Good technical support from the GP lab will also help in the process. It is of utmost importance that we have a good trial lens set from a reliable laboratory from which we can perform customized fits for these challenging cases. Our most important asset, however, is our expertise and our capacity to see solutions where others may not. CLS

| Mr. Bastos is the director and clinical instructor on contact lenses at the Instituto de Olhos Dr. Saul Bastos (IOSB) and the director of Ultralentes, a GP lab focused on scientific research of specialty GP lens designs in Porto Alegre, RS, Brazil. |