


CORRECTING PRESBYOPIA
Improving Vision Outcomes For Presbyopic Patients
A new way to measure visual quality with multifocal contact lenses may help improve vision for presbyopes.
By Bill Reindel, OD, MS; Gerard Cairns, PhD, MCOptom, FAAO; & Paul China, OD, FAAO
A recent global survey of 3,800 vision-corrected subjects found that vision was the most compelling feature they considered when choosing eye-related products. When broken down by refractive error type, vision remained the most compelling feature for presbyopic patients (Market Probe Europe, 2009).
Today's presbyopic contact lens wearers are a growing population who seek improved near vision without distance vision compromise. They want the convenience of contact lens wear without the hassles of compromised vision (Bennett, 2008; Morgan and Efron, 2009). The enhanced optics of new contact lens designs considerably reduce problems encountered with previous multifocal contact lenses; however, multifocal lens designs have optical characteristics that can produce secondary or “ghost” images.
Objective measurements of vision do not always align with subjective reports by patients. For instance, while various designs of simultaneous vision lenses perform similarly on standard clinical tests (Situ et al, 2003), such as high-contrast visual acuity at distance and near, patients may still mention differences in their vision. Improved testing allows qualification as well as quantification of differences in vision that cannot be measured via standard clinical tests.
The purpose of this study was to compare distance vision with two unique simultaneous vision multifocal designs using standard visual acuity measures and a novel method to measure secondary images.
A New Way to Assess Vision With Multifocal Lenses
This study compared differences in logMAR visual acuity and vision quality between PureVision Multi-Focal (Bausch + Lomb [B+L]) lenses and Acuvue Oasys for Presbyopia (Vistakon). Twenty-two presbyopic patients requiring reading addition powers from +0.75D to +2.50D who had a mean age of 53.2 ± 5.8 years and a mean near add of 1.81D ± 0.40D were examined. Subjects were masked during the study. Approval was obtained from the Southwest Independent Institutional Review Board (Fort Worth, Texas), and investigators obtained written consent from each patient prior to testing.
After undergoing a spherical refraction of both eyes, subjects applied a randomized Test and Control lens-pairing onto their eyes, with each lens selected according to the respective manufacturer's recommendations. After allowing the lenses to settle for 3 minutes, investigators assessed the lens fit, performed a spherical over-refraction, and performed all tests monocularly while patients were viewing through the over-refraction. Distance logMAR visual acuity was measured in high and low illumination, and near visual acuity was measured in high illumination. Patients rated visual quality and comfort on a visual analog scale ranging from 0 (poor) to 100 (excellent).
To examine the visual differences that patients may notice, investigators used a novel technique to test secondary images. This can be a useful way to compare the changes in vision that patients notice but may not be detectable using standard clinical tests. For this procedure, the subjects fixated on a projected 22-mm spot of white light at 6 meters. Using a laser pointer, they indicated the outermost edge of any secondary images. The investigators recorded the position from the edge of the spot of white light.
Differences Observed Between Lens Designs
When tested using the novel procedure described above, the PureVision Multi-Focal lenses exhibited significantly fewer secondary images compared with the Acuvue Oasys for Presbyopia lenses (p<0.02). The mean values from the edge of the circle were 21.4mm ± 12.3mm for the PureVision Multi-Focal and 35.8mm ± 24.9mm for the Acuvue Oasys for Presbyopia lenses. Figure 1 illustrates the extent of the secondary images. The Acuvue Oasys for Presbyopia lenses exhibited approximately 67 percent greater extent of secondary images from the edge of the circle.
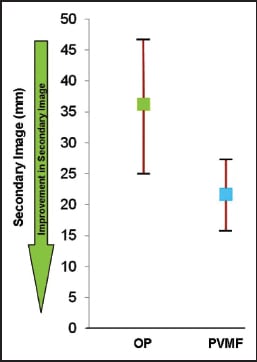
Figure 1. Mean secondary image at 6m for each lens. OP = Acuvue Oasys for Presbyopia. PVMF = PureVision Multi-Focal.
Although there were no significant differences between the two lens types for mean-normalized distance high-contrast/high-illumination and high-contrast/low-illumination visual acuity, the visual quality rating (measured on a visual analog scale) was significantly better for the PureVision Multi-Focal when compared with ratings for the Acuvue Oasys for Presbyopia at distance (p<0.01). The mean difference for distance visual quality ratings was lower for the Acuvue Oasys for Presbyopia lens, with Acuvue Oasys for Presbyopia lenses and Pure-Vision Multi-Focal lenses demonstrating means of 60.0 ± 20.7 and 74.4 ± 15.8, respectively (Figure 2). There was no significant difference in mean comfort ratings between the PureVision Multi-Focal (93.3 ± 10.0) and the Acuvue Oasys for Presbyopia (96.0 ± 4.6).
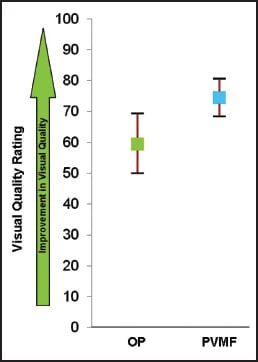
Figure 2. Mean (± SD) visual quality rating 6m for each lens. OP = Acuvue Oasys for Presbyopia. PVMF = PureVision Multifocal.
There was a preference trend for PureVision Multi-Focal (p=0.056). Thirteen subjects preferred the PureVision Multi-Focal lens, five subjects preferred the Acuvue Oasys for Presbyopia lens and four subjects had no preference. Twelve of the 13 subjects who preferred the PureVision Multi-Focal lens listed “vision” as a reason, indicating the importance of clear vision to patients.
Discussion
To meet the demands of patients and practitioners, contact lens manufacturers offer multifocal options using a variety of design characteristics. Two commonly used options are aspheric optics, which allow for a smooth transition in powers across lens geometry, or distinct optical zones, which alternate powers between distance and near.
Imaging techniques can be used to help visualize refractive differences induced by various optical designs. One such technique is Phase-Shifting Schlieren images. This method can be used to visualize variations in optical power across the optic zone of a contact lens. Specific, discrete power zones that are present in a multifocal contact lens become quite apparent.
The Schlieren images in Figure 3 are useful in depicting sharp transitions in power across the optic zone that may influence overall optical quality. The measurement of secondary images by contact lens wearers offers a sensitive method to quantify light deviations and vision quality associated with varying multifocal designs.
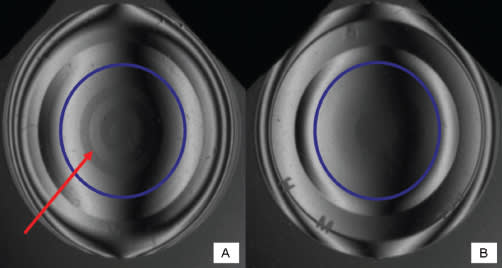
Figure 3: Phase-Shifting Schlieren images of (A) −3.00D Oasys for Presbyopia +1.75D Add and (B) PureVision Multi-Focal High Add. The blue circle denotes the optic zone of the lenses. The red arrow indicates where a transition in power occurs on the lens.
Although clinical tests, such as visual acuity, do not always distinguish between multifocal lens types, subjective preferences and new measurement techniques can help evaluate multifocal options for patients. The new test described here provides a method to quantify vision information that may not be detected by measuring visual acuity. As a result, this new technique may help to determine which patients are more likely to succeed with various multi-focal contact lens designs.
Comparison of PureVision Multi-Focal and Acuvue Oasys for Presbyopia lenses showed no differences in visual acuity at distance or near, but patients subjectively preferred the visual quality at distance provided by the PureVision Multi-Focal lenses. The patients' preference for the PureVision Multi-Focal contact lens may be explained by the greater secondary images experienced while wearing the Acuvue Oasys for Presbyopia contact lenses.
Conclusion
This method for quantifying secondary images revealed significant differences between the PureVision Multi-Focal and the Acuvue Oasys for Presbyopia lens designs that were not discerned with distance visual acuity measures. Reduced secondary images with the PureVision Multi-Focal lens can play a significant role in patients' acceptance of presbyopic contact lens correction. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #192.

| Dr. Reindel is the director of Medical Affairs for the global vision care business of Bausch + Lomb. |

| Dr. Cairns is manager, Global Medical Affairs for Bausch + Lomb. |

| Dr. China is Pharmaceutical Clinical Life Cycle Manager at Bausch + Lomb. |