


Contact Lens Care & Compliance
Handling and Care of Scleral GP Contact Lenses, Part 1

By Susan J. Gromacki, OD, MS, FAAO
The more frequent use of scleral GP lenses is a recent occurrence, and as such, there is little written on their handling and care. Many of the most frequently used contact lens textbooks were published before the lenses' re-emergence. Moreover, there is not a currently agreed-upon standard of care for these lenses.
In this column I'll begin the discussion of the handling of these lenses. I'll provide information on scleral lens care in an upcoming column.
A Scleral Lens Overview
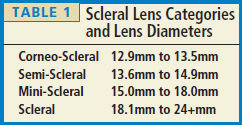
Due to their large diameters and how they're fit, scleral lenses require specific handling and care instructions. Scleral GP lenses measure between 12.9mm and more than 24mm in diameter and are subdivided into four categories (Table 1; Sindt, 2008).
The modality provides a healthy, stable fit for irregular corneas by resting primarily on the sclera, bridging over the cornea and bathing it in tears. New manufacturing technologies have improved reproducibility and reduced cost, and with new oxygen-permeable materials, the threat of hypoxia that previously plagued this modality has virtually been eliminated. As a result, the category of lenses has grown exponentially.
The Scleral Lens Solution Survey (van der Worp, 2010) illustrates that there is no current standard of care. Of 46 scleral-lens-fitting respondents worldwide, 72 percent prescribed GP care solutions for lens storage, 48 percent peroxide, and 17 percent soft lens solutions (respondents were allowed to select more than one option). For lens application, 72 percent recommended non-preserved saline solution; 22 percent GP lens care solutions; 7 percent soft lens care solutions; 7 percent preserved saline; and 28 percent other (primarily artificial tear supplements, according to the author).
Handling Tips
Scleral lenses need to be filled with ophthalmic solution before application. The Scleral Lens Solution Survey found that most practitioners recommend nonpreserved saline solution for this purpose, even though this is still technically an off-label use in the United States. Because scleral lenses provide minimal tear exchange, contact with any substance behind the lens is prolonged as compared to a corneal GP contact lens. Thus, it is advised to refrain from exposing the cornea to preservatives or buffers that may induce allergic or hypersensitivity reactions (Sindt, 2011). Caution patients, however, not to soak their lenses overnight in nonpreserved saline. It does not provide disinfection and increases the potential for microorganism growth (van der Worp, 2010). Educate your patients about potential contamination within a bottle of nonpre-served saline. Instruct your patients to dispose of the bottle on or before its expiration date or if its tip comes in contact with any surface.
To eliminate contamination risk, many practitioners prescribe unit-dose 0.9% NaCl inhalation/irrigation nonpreserved saline supplied in 3ml or 5ml vials. This also is an off-label use in the United States. The solution is free of preservatives and buffers and can be purchased online or at most pharmacies (DeNaeyer, 2011; Sindt, 2011). CLS
For references, please visit www.clspectrum.com/references.asp and click on document #191.
Dr. Gromacki is a Diplomate in the Cornea, Contact Lenses, and Refractive Technologies section of the American Academy of Optometry. She is chief research optometrist at Keller Community Hospital in West Point, N.Y.