


SEMI-SCLERAL LENSES
Semi-Scleral Applications for Healthy Eyes
From part-time wear to myopia progression, these lenses should be a staple in your armamentarium.
By Jason Jedlicka, OD, FAAO; Marsha M. Malooley, OD, FAAO; & Renee E. Reeder, OD, FAAO
Scleral lenses are another tool in your contact lens toolbox, but their application is far more reaching than simply for patients who have compromised corneas. As the five following cases illustrate, semi-scleral lenses provide improved comfort and clear vision to patients who are new or returning to contact lens wear for a variety of reasons.
Case 1: Returning to GPs
Our first case is a 47-year-old female with a history of high myopia, astigmatism, and presbyopia as well as ocular allergies. She had worn GP lenses for many years with great vision and tolerability, but in recent years suffered from chronic red eyes and had switched to soft torics in an attempt to help abate the redness. While the redness was improved, and her comfort with the soft torics was good, she never felt that the vison quality was as good as it was with her GPs.
At the patient's evaluation, her entering distance acuity with her soft toric lenses was 20/40 OD and 20/30 OS. Her near acuity was measured at 20/40 OD and 20/30 OS with just her contact lenses. She did not typically use additional correction for near vision. The lens fit was acceptable with slight lens rotation in each eye. Over-refraction of the contact lenses was OD −0.50 +0.75 x 115, 20/20 and OS −1.00 +0.50 x 135, 20/20−2. Slit lamp examination revealed a clear cornea with trace injection of the conjunctiva OD and OS.
After removing the lenses, her manifest refraction was OD −15.25 +2.50 x 86, 20/20 and OS −12.50 +2.50 x 94, 20/20. Keratometry was performed with readings of OD 45.00 x 47.75 @ 85 and OS 44.75 x 47.00 @ 95. Her near add was measured at +1.50D. All other examination findings were normal.
We discussed options for vision correction, which included: multifocal spectacle lenses; continuing in her soft lenses and trying to optimize vision with adjustments to the lens powers (which might require reading glasses or multifocal lenses); returning to GP lenses in either multifocal, monovision, or distance-only format (which could include corneal lenses); hybrid lenses; or larger-diameter lens designs. After discussing the options, she preferred not to use glasses as her primary mode of correction. She was also somewhat frustrated by the vision with soft toric contact lenses and had tried adjusting them in the past with little success. While she enjoyed the vision with GP lenses, she was not excited about returning to them due to the redness and discomfort she had experienced.
Trying a corneo-scleral lens design was very appealing to our patient because she liked the idea of GP lens vision with more comfort. We explained that part of the problem with her old GP lenses may have been poor blinking due to lens awareness, which made her eyes red from dryness, and that using a larger lens would significantly decrease lens awareness, help her perform complete blinks, and minimize the likelihood of redness. We also told her that by using a multifocal design, we could likely improve both her distance and near vision without the need for reading glasses. After this discussion, she was ready to give them a try.
We proceeded with a trial fitting of So2Clear Corneal Scleral lenses (Dakota Sciences/Art Optical). Due to her steep but smaller corneas, the lens with the best fitting sagittal depth was the 44.00D lens OD and OS. With an over-refraction, the vision was corrected to 20/20 in each eye with a final power of −9.25 OD and −7.75 OS. The diameter chosen was 13.8mm for each lens. The add zone utilized was 2.25mm in each eye with a power of +1.25D.
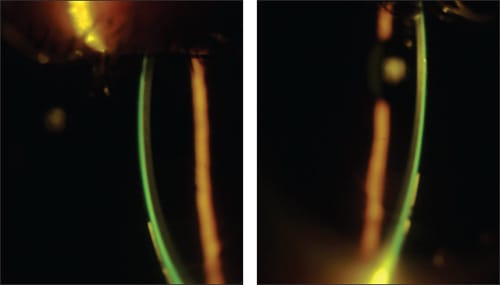
At the dispensing appointment, we applied the lenses and allowed them to settle. After settling, fluorescein was instilled into each eye and was allowed to circulate under the lenses. The fit was acceptable and the comfort was good (Figures 1 and 2). Distance vision was measured at 20/20 OD and 20/25 OS, with near vision at 20/25 OD and OS. The patient reported the comfort to be excellent with no real lens awareness. We dispensed the lenses with instruction for application, removal, care, and handling. She returned for a subsequent follow-up visit at which time she reported improved vision and no issues.
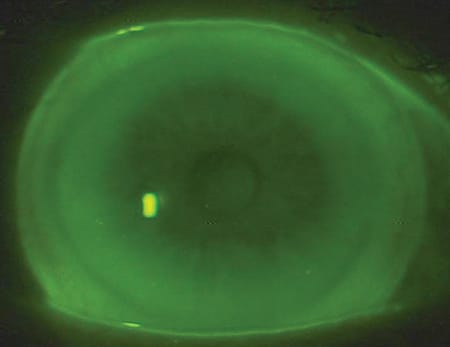
Figure 1. Case 1 So2Clear corneo-scleral lens OD.
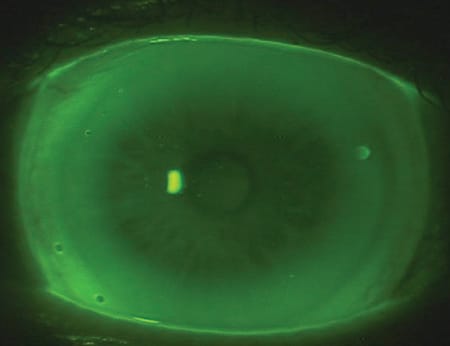
Figure 2. Case 1 So2Clear corneo-scleral lens OS.
We have evaluated this patient at annual eye examinations since the initial fitting three years ago, and she continues to have good comfort and vision with the corneo-scleral lenses. Lens powers have been updated to accommodate changes in prescription, but otherwise no significant changes have been required.
Case 2: Lenses for Part-time Wear
Our second case is a 45-year-old male with a history of moderate myopia and astigmatism. He leads a very active lifestyle and is a professional drag racer. He presented for an eye examination using spectacles only with an interest in resuming contact lens wear. He had stopped wearing lenses due to poor quality vision and what he considered poorly fitting lenses.
At his initial presentation, his spectacle visual acuity was 20/20 in each eye. He had just obtained new glasses, and the correction in the lenses was neutralized to be OD −4.25 −0.50 x 165 and OS −2.50 −0.75 x 20. He was not using a bifocal at this time but removed his glasses for near work as needed. All entrance testing, including pupils, extraocular muscles (EOMs) and confrontation fields were normal. Keratometry was performed with readings of OD 42.75 x 43.25 @ 75 and OS 42.75 x 43.37 @ 105.
A refraction was completed with no change found compared to his new glasses. A slit lamp examination was unremarkable, as was the remainder of the ocular health assessment. Of note, it was clear by simple observation that he had larger corneal diameters compared to the average patient.
After completing the examination, we discussed his options. His primary interest was clear vision and stability of fit, and his plan was to use the lenses on a part-time basis for recreational activities and driving. We discussed how GP lenses could offer the best quality of vision, but to stay adapted and comfortable with the lenses might require more wear than he had planned. Additionally, corneal lenses would not necessarily provide the stability of fit he desired. Soft lenses were also an option, although with his larger corneal diameter and desire for clear vision, we would have needed a custom soft toric design. In this instance, with the GP optics and the ability to wear lenses part time, as well as the customized fit parameters, a corneo-scleral lens seemed to be a good choice. He consented, and a fit was undertaken.
We opted to try a So2Clear Corneal Scleral lens as our first trial. Using the initial fit guide, we chose a lens of base curve 43.00D for each eye, with an overall diameter of 14.0mm. It was clear from the initial lens placement that a larger lens diameter would be needed. As is also often the case with larger corneal diameters, a much deeper lens than would otherwise be predicted was required. We next applied a 44.00D base curve lens on each eye, which also proved to be too shallow. Finally, a 45.00D base curve lens appeared to provide acceptable sagittal depth to properly land the edge of the lens on the sclera. However, the lenses demonstrated poor midperipheral vault, so we initially ordered OD So2Clear 43.00D base curve, 45.00D peripheral system, 15.0mm diameter, −5.00D power in Boston XO2 (Bausch + Lomb [B+L]) with fenestration (Figure 3) and OS So2Clear 43.00D base curve, 45.00D peripheral system, 15.0mm diameter, −3.00D power in Boston XO2 with fenestration (Figure 4).
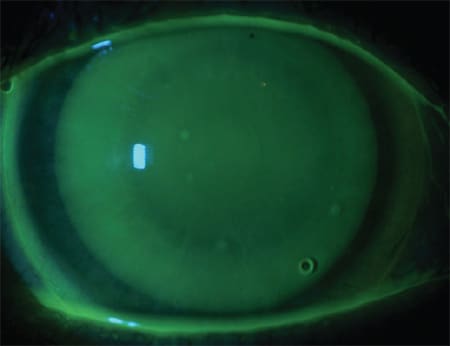
Figure 3. Case 2 So2Clear corneo-scleral lens OD.
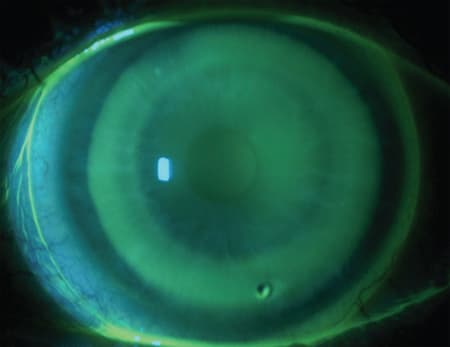
Figure 4. Case 2 So2Clear corneo-scleral lens OS.
The dispensed lenses provided excellent comfort and fit, with visual acuities of 20/20 in each eye. The patient was instructed on application and removal as well as care and handling, and he managed to demonstrate good technique. He wore the lenses on a part-time basis, returning for a follow-up visit with no problems two weeks after the initial dispensing. He continues to use the lenses during recreational activities such as racing and boating.
These first two cases demonstrate the value of GP lens optics for patients who have astigmatism and a desire for clearer vision. While standard GP lenses or soft toric lenses can be and usually are utilized in these situations, larger-diameter GP lenses can offer many advantages. Clearer vision, good initial comfort, the option for occasional wear, and customized parameters can provide an optimal outcome for many patients versus their other options. While many of us have been steadily utilizing these larger-diameter lenses for irregular corneas, we certainly should not neglect their possibilities for our normal cornea population.
Case 3: Dry Eye and Better Comfort
A 57-year-old white female presented for an examination to explore contact lens options. She complained of contact lens intolerance. The patient had started with hard contact lenses at age 12 and later switched to GP lenses, with successful lens wear until her early 50s. She reported that her eyes had become progressively more dry over the past several years, and she tried Restasis (Allergan) for about 12 months with no improvement in her symptoms. After discontinuing Restasis, her previous eyecare practitioner inserted punctal plugs. She was refit into soft toric contact lenses with better lens comfort but poor vision. Her last eye examination was approximately 15 months ago, and she had not worn any contact lenses since that time.
Her examination findings were refraction OD −9.75 −1.25 x 050, 20/20, add +2.50 J1 and OS −11.00 −1.75 x 145, 20/20, add +2.50 J1. Keratometry readings from topography (Figures 5 and 6) were OD 44.50/43.00 @ 44; OS 45.13/43.89 @ 146.
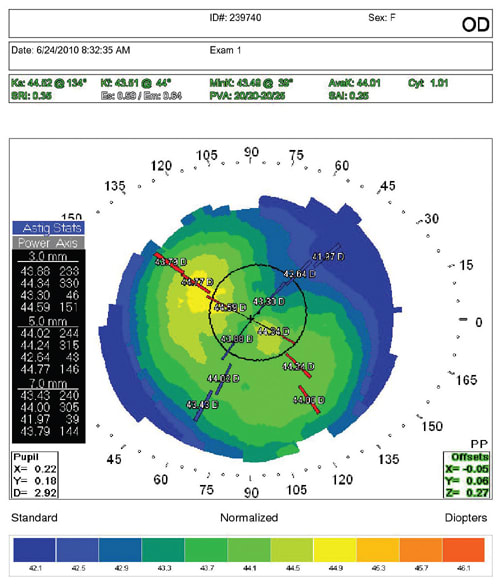
Figure 5. Case 3 K readings from topography OD.
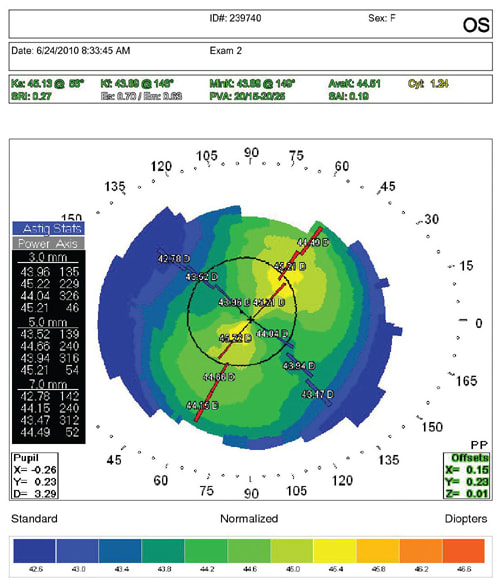
Figure 6. Case 3 K readings from topography OS.
During refraction and trial framing, it was apparent that the patient was very sensitive to changes or reduction in her astigmatism. Anterior segment evaluation revealed no punctal plugs present, 1+ meibomian gland dysfunction OD and OS, mild conjunctival chalasis OD and OS, and a clear cornea free of corneal staining OD and OS.
After discussing contact lens options with her, we performed a diagnostic contact lens fitting using the MSD (Mini Scleral Design) lens by Blanchard Contact Lens. A 4.20 sag lens was selected as the starting trial for both OD and OS. The fitting set has only one lens of each parameter. To decrease chair time, a Standard profile curve was applied OD and an Increase profile curve was applied OS.
The diagnostic lens parameters were OD MSD design, 4.20 sag, 15.8mm diameter, plano power, standard non-fenestrated profile curve, over-refraction of −9.25D resulted in 20/20−; OS MSD design, 4.20 sag, 15.8mm diameter, plano power, Increase non-fenestrated profile curve, over-refraction of −10.25 resulted in 20/20−.
Upon trial evaluation the lens OD demonstrated even corneal clearance free of corneal bearing (about 25 percent of corneal thickness or 125µm), limbal clearance, and no conjunctival vessel blanching. The evaluation OS revealed even corneal clearance free of corneal bearing similar to OD, a C-shaped bubble along the limbal region, and no conjunctival vessel blanching.
The patient reported good vision and comfort OD and OS and was pleased at the opportunity to try a new type of contact lens. We explained fitting fees, lens costs, and the fitting process to her. We also emphasized the need for reading glasses over the lenses because the contact lenses would correct distance vision only. Patient expectations were addressed. She stated she would be happy with part-time wear with an average wear time of about eight hours.
We ordered the following non-fenestrated lenses for the patient based on the initial diagnostic fitting: OD MSD design, 4.20 sag, 15.8mm diameter, −8.50D power, Boston XO (B+L) material, Standard profile curve, no peripheral edge adjustments; OS MSD design, 4.20 sag, 15.8mm diameter, −9.25D, Boston XO material, Standard profile curve, no peripheral edge adjustments.
The patient returned for application and removal training and was given Boston Simplus Multi-Action Solution (B+L) for cleaning and soaking with Unisol 4 preservative-free saline solution (Alcon) for lens application. A small non-ventilated plunger was used for lens removal. She was instructed to build up her wearing time starting with two hours the first day, increasing by two additional hours each day.
She returned to the clinic for her contact lens check visit four days later with complaints of fogging vision after four hours and a “tight” feeling upon lens removal. The lenses felt “suctioned” to her eyes. The patient reported wearing the contact lenses for six hours prior to her appointment. Lens evaluation revealed about 1mm of conjunctival vessel blanching at the edge of the lens OD and OS with some debris in the tear film under both lenses. Her visual acuity (VA) measured 20/25 OD and 20/25 OS. Anterior segment evaluation showed a clear cornea OD and OS, with partial conjunctival impression rings OD and OS. In addition, the patient inquired about adjusting one lens to help with computer/cell phone clarity. After discussing monovision, a +1.00D loose lens was held over her non-dominant left eye, which allowed her to see J2 at about 18 inches. We reordered the contact lenses with the following parameters: OD MSD design, 4.20 sag, 15.8mm diameter, −7.75D, Boston XO material, Increase profile curve, 1 flat peripheral curve; OS MSD design, 4.20 sag, 15.8mm diameter, −7.75D, Boston XO material, Increase profile curve, 1 flat peripheral curve.
The patient returned two weeks later for a contact lens dispensing visit. VA with the new lenses measured OD 20/20− and OS 20/50. Her near vision OU was J2. Over-refraction was plano OD and −1.00 OS.
She returned two weeks later and reported good distance and intermediate vision. Comfort was good OD and OS, and she experienced no problems with lens application or removal. She was wearing +1.25D over-the-counter reading glasses over the contact lenses as needed. Her average wearing time was 12 to 14 hours about five days per week. Upon evaluation the contact lens OD demonstrated no vessel blanching, full limbal clearance, and no corneal bearing. Evaluation OS showed no vessel blanching, minimal limbal clearance, and no corneal bearing. There was some mild conjunctival chemosis OS near the limbal region at about 7 o'clock. After discussing the case with a consultant, it was recommended to change the left lens to a double increase profile curve.
After dispensing and wearing the new left lens for about two weeks, she reported good comfort, vision, and overall satisfaction. Vision remained OD 20/20 OS 20/50 with J2 at near. Corneas were clear OD and OS, limbal clearance improved OS, and the conjunctiva was white and quiet OD and OS.
Scleral and mini-scleral contact lenses may not be your first lens choice for patients; however, they have definitely earned a place in our practices. The same visual benefits of corneal GP lenses apply to scleral contact lenses, but with improved patient comfort and lens tolerance. With an increase in the number of mini-scleral lens designs and availability of diagnostic lens sets, practitioners are experiencing increased success fitting these larger-diameter lenses. Mini-scleral lenses no longer need to be reserved for only the most complicated irregular corneas. Do not be afraid to think out of the box and explore mini-scleral designs on even your normal healthy patients who may not have been successful in the past with other contact lens options. Patients will appreciate a fresh approach to correcting their vision and a chance to join the ranks of other successful contacts lens wearers.
Case 4: Myopia Progression
A 14-year-old African American female presented to the clinic with a −1.50D increase in myopia in less than a year while wearing soft contact lenses. Her family history was significant for myopia. Due to the large progression, she was sent for blood work, and diabetes was ruled out.
Her spectacle prescription was OD −5.75 −0.75 x 007 and OS −5.00 −1.00 x 180, which provided visual acuities of 20/20 in both eyes. She was initially fit with standard-diameter GP contact lenses, which provided excellent vision, but the patient rated their comfort as a 2 out of 10. Despite her desire to return to soft lenses, her parents were eager to maintain GP lens wear in hopes of minimizing any further progression of her myopia. After lengthy discussion, it was decided to try a corneo-scleral contact lens to provide her with improved comfort.
Her topographies (Figures 7 and 8) showed a healthy cornea with mild with-the-rule astigmatism. We ordered So2Clear contact lenses in these parameters: base curve 7.42mm (45.50D), power −5.75D, overall diameter (OAD) 14.0mm; standard peripheral curve.

Figures 7 and 8. Case 4 regular corneal topographies with horizontal visible iris diameter.
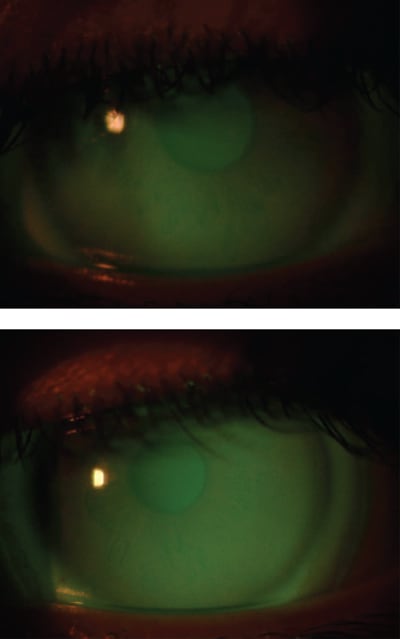
The lenses aligned with the cornea, cleared the limbus, and landed on the sclera evenly. The patient reported that she could barely feel the lenses and gave them a 9-out-of-10 comfort rating. Upon dispensing, the lenses fit well (Figures 9 and 10) and provided excellent vision. She has now been wearing this contact lens design for two years with less than 0.50D change in refraction.
Figures 9 and 10. Case 4 optic section of the lenses showing alignment over the central cornea.
Case 5: More Myopia Progression
A 15-year-old African American female presented to the clinic wearing spectacles and wanted to improve her vision with contact lenses. Her spectacle prescription was −1.25 −3.25 x 007 OD and −2.00 −2.25 x 180 OS, which provided 20/20 visual acuity in both eyes. The cost of extended range toric contact lenses was concerning to the patient's family. We offered to let her participate in a student workshop for GP lenses. Her topographies (Figures 11 and 12) were taken and e-mailed to the laboratory. The sim K readings revealed moderate astigmatism of 39.50/43.37 OD and 40.12/43.12 OS. The patient's horizontal visible iris diameter was 10.5mm. Both So2Clear lenses and bitoric lenses were designed.

Figures 11 and 12. Case 5 corneal topographies with horizontal visible iris diameter, demonstrating high regular with-the-rule astigmatism.
At the workshop, the patient found the bitoric GP lenses intolerable. They were immediately removed and replaced with the So2Clear lenses. She found these lenses markedly more comfortable and reported better vision. Due to her small corneas, the lenses were a 13.1mm diameter. The initial base curve for the right eye was 8.28mm with a power of −2.50D with standard peripheral curves. The left lens had an 8.21mm base curve with a power of −3.00D and standard peripheral curves. Slit lamp evaluation of the lenses showed superior temporal pooling and blanching at the edge of the lenses (Figures 13 and 14).
Figures 13 and 14. Case 5 overall view of the lenses with full corneal coverage.
The lenses were ordered 1.25D flatter base curve in the right eye and 0.75D flatter base curve in the left eye. They were also ordered with a 1.00D flattening to the peripheral curve system to eliminate the minor blanching noted. Flatter lenses were then chosen with a base curve of 8.55mm, power of −1.00D, OAD of 13.1mm, and 1.00D flat peripheral curves for the right eye and a base curve of 8.35mm, power of −1.75D, OAD of 13.1mm, and 1.00D flat peripheral curves. (Figures 15 and 16)
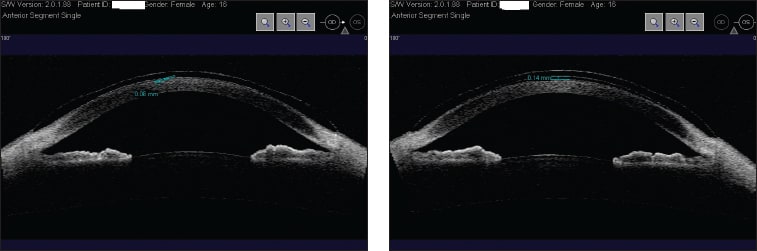
Figures 15 and 16. Optical coherence tomography images of the lenses in Case 5. The images demonstrate the alignment of the lenses with the smallest amount of clearance between the lens and the cornea.
The new pair aligned centrally with no impingement on the conjunctiva. The patient reported crisp vision and good comfort. After more than two years, her prescription is unchanged.
There are many options for cosmetic lens fitting of patients who have significant refractive error. While the mainstream for many of these cases is frequent replacement or disposable soft lenses, corneo-scleral lenses can offer enhanced vision, equivalent comfort, and excellent oxygen transmission and health. They also may be successfully ordered empirically for regular corneas—minimizing chair time and maximizing profitability. In the two previous cases, they also appear to have aided in stabilization of myopic progression. CLS
 |
Dr. Jedlicka is owner and director of the Cornea and Contact Lens Institute of Minnesota. E-mail him at jgjod@yahoo.com. |

|
Dr. Malooley is part of an MD/OD practice and adjunct assistant professor at the Illinois College of Optometry. E-mail her at marsham@chicagocornea.com |

|
Dr. Reeder is the chief of the contact lens service at the Illinois College of Optometry. She is a consultant/advisor to B+L and Ciba Vision. She has received research funding from Metro Optics and lecture honoraria from Alcon. E-mail her at rreeder@ico.edu. |