


FITTING GP LENSES
The GP Decision-Making Process
From patient selection to lens design, see why today's GP lenses are as easy to fit as soft lenses.
By Edward S. Bennett, OD, MSEd, FAAO
Gas permeable (GP) contact lenses can provide excellent optics to astigmatic, hyperopic, myopic, and presbyopic patients. This article will guide you through the decision-making process for GP lenses, from patient selection to material and design choices.
Patient Selection
The easy rule to remember for selecting patients for GP lenses is that anyone who is a good candidate for contact lenses should be a good candidate for GPs. Patients who have dry eye likely won't be good candidates for any contact lens—soft or GP—until the dry eye is properly managed. If a patient is a good candidate for contact lenses, is motivated, and is given the opportunity to try GPs, there's a good likelihood that the patient will end up wearing GPs.
Practitioners are reluctant to give patients the opportunity to wear GP lenses because they are concerned about initial lens comfort. It is important to understand that today's designs are more initially comfortable compared to those in the past. Larger-diameter lenses move much less on the eye and decrease the initial awareness that patients feel with the movement of the lens. Today's GP lenses are also more comfortable because most utilize ultra-thin designs that have significantly less mass. An aspheric or pseudo-aspheric periphery provides even lens clearance, helping with comfort and centration. Past designs allowed for inferior decentration, which creates comfort and vision problems and can cause dryness.
Astigmatic Patients Today, one of the biggest challenges in prescribing contact lenses to astigmats is attempting to fit all astigmats into soft toric lenses. Astigmatic patients deserve the opportunity to have a choice. Many soft toric patients are not pleased with their vision. There is no argument that soft toric designs have improved dramatically, but GP lenses provide superior vision, especially to patients requiring a toric correction. GPs have a good optical surface, do not absorb water, and automatically neutralize the astigmatism of the anterior cornea. Toric GPs should be the lens of choice for high astigmats—those who have 2.50D or more of astigmatism—because you can achieve a higher quality of vision than with soft lenses.
High Myopia and Hyperopia High myopes can benefit from GPs in several ways. Plus lenticular application can control the edge thickness; therefore, the overall mass is reduced and there is less likelihood for inferior decentration. Hyperopes can achieve very good oxygen transmission with high- and hyper-Dk materials and, as with high myopes, there are no concerns about the peripheral cornea.
Presbyopia In answering consumer questions on www.contactlenses.org, the most common question I respond to pertains to GP multifocals. Consumers are wondering whether GP multifocals are a viable choice for them; many people write, “My doctor said GP multifocals are not a good option.” Manufacturers know that presbyopes are looking for better vision, and the GP lens market has been stable over the past few years due to the increase in GP multifocal designs.
Studies have shown that the quality of vision as well as the success rate of GP multifocals is very good (Byrnes and Cannella, 1999; Remba, 1988). When compared to soft multifocals and monovision, the quality of vision with multifocal GPs is significantly better than that with both of those modalities (Rajagopalan et al, 2006). According to Contact Lens Spectrum Editor Jason Nichols, OD, MPH, PhD, FAAO, practitioners' number-one presbyopic correction preference today is multifocals, not monovision (“Contact Lenses 2010,” January 2011 issue).
Advantages of GP multifocals are:
• Non-water-absorbing
• High optical quality
• Good, if not excellent, vision in all distances
• High-add aspheric designs
• Segmented translating designs
This last advantage is important because few soft translating designs exist. Having segmented translating designs in your toolbox helps when your presbyopic patients require excellent distance as well as near vision. For patients who want uninterrupted vision, these designs are your best option.
There's no doubt that GP lenses are fit less frequently than they should be in practice and much less than what would be optimum for patients. The primary reason for this is initial awareness—not only awareness by the patients, but practitioners' fear of patients' initial awareness. To help mitigate this, remember when presenting this option to patients to say “awareness” rather than “discomfort” and “GP” rather than “rigid.”
The next most common reason to avoid fitting GP lenses is the concern about chair time. Good news: with improvements in GP designs and technology as well as in how we approach patients, chair time for GPs is about the same as that of soft lenses, and initial lens awareness is less.
Lens Material Selection
The most common question that laboratory consultants hear is, “What material should I use?” This is understandable given the large number of materials available today. Historically, materials in a rigid plastic format began with polymethylmethacrylate (PMMA), and PMMA lenses are still manufactured and dispensed today. The reason is because in some practitioners' minds, don't fix it if it's not broken. I say it is broken. Every cornea wearing a non-oxygen-permeable material becomes edematous.
Silicone acrylate (SA) materials, introduced in 1979, had the advantage of oxygen permeability and are still being used today. The challenge with SA materials is their hydrophobic tendency. As the amount of silicone and thus oxygen permeability in the materials increased, the lenses became less wettable, less stable, and prone to flexure and warpage.
In the mid-1980s, fluorosilicone acrylate (FSA) materials were introduced. The addition of fluorine helped both wettability and oxygen permeability. FSA lens materials have been the standard of care for more than 25 years. More recent FSA materials have been able to reduce the hydrophobic effect of the silicone content and maintain good oxygen permeability due to changes in the material composition. These newer materials are also more durable and flexure-resistant compared to their FSA predecessors.
So what material do you use? First, know that all FSA materials available today are successful. Second, the consultants at your Contact Lens Manufacturers Association (CLMA) member laboratories are excellent resources for recommending one or more materials to you. Some designs are available only in certain materials, which helps to narrow down the choices. Other useful tools are the Materials Guide collated by the GP Lens Institute (GPLI), which is available at www.gpli.info and lists all materials made by button manufacturers, and the July 2007 GP Insights column by Marjorie J. Rah, OD, PhD, FAAO, titled “A GP Materials Guide,” which discusses GP material selection.
In making my selection, I divide materials by their oxygen permeability (Dk) values: low, high, and hyper Dk. Low-Dk materials have values of 25 to 50. Because of their stability and wettability, I recommend low-Dk materials for all daily wear myopes. High-Dk materials have values of 51 to 99. I suggest high-Dk materials for hyperopes and high myopes because—on average—a plus power lens is twice as thick as a minus lens, and twice the oxygen permeability will be needed. For myopes interested in extended wear, I prescribe those materials approved for that schedule. Hyper-Dk materials have a Dk of 100 or greater. Some practitioners choose hyper-Dk materials for every patient to optimize the corneal physiological environment. I prefer lower-Dk materials for daily wear patients because of their flexure resistance and longevity. Laboratories today are able to produce an ultrathin design in a low-Dk material that will still provide reasonable flexure resistance. Such a lens will have less mass and achieve a good fitting relationship—remember that as the lens gets thicker, it's more likely to decenter inferiorly.
The key factor in material choice is wettability. Remember that some hyper-Dk materials offer good surface wettability; it's not a rule that as the Dk goes up, the surface wettability goes down. One of the most significant recent gains in GP lens materials has been an overall improvement in surface wettability. If a lens exhibits good surface wettability and keeps the tear film in contact with the lens over a period of time, the tear film is less likely to dry out. It is apparent that we don't see corneal desiccation (3 o'clock and 9 o'clock staining) as much as we did 20 years ago, and an important factor in this (in addition to improved centration due to less mass) is better lens surface wettability.
Another frequent question pertains to plasma treatment. Should you order your lenses plasma-treated? Many laboratories have adopted this treatment process, so plasma-treated lenses are becoming more popular. The plasma treatment is not a coating; it is a treatment in which the front surface of the lens is cleaned of all manufacturing residue. Plasma treatment can initially enhance surface wettability and result in slightly better initial comfort (Bennett, 2006). We don't know how long plasma treatment lasts or what compromises it. Abrasive cleaners and polishing the lens surface likely reduce the beneficial effects of plasma treatment.
Bottom line: as long as you're choosing an FSA material, consider fit and design first. Fit is more critical than the specific material. Many multifocal and irregular cornea designs are available in only certain materials, so design will drive your material choice in some cases. If a laboratory chooses a specific material for a certain design, it is very likely that the material is appropriate for that design.
Lens Design and Fitting
It's important to recognize that today the GP fitting process is easier, more streamlined, more efficient, and more successful compared to how we approached it 20 years ago. We now have lenses that are easier to fit, initially more comfortable, and that require less chair time than their predecessors did. Materials provide better initial wettability, and designs optimize centration and align well with the eye. It is now a common practice to use a topical anesthetic prior to the first lens application to help reduce the anxiety of both practitioner and patient regarding initial awareness of the lens.
The most important benefit of GP lenses is vision. If the first lens that you apply is in a patient's prescription, the patient will likely experience the “wow” factor that GPs provide. The patient will be aware of the lens if he hasn't worn GPs before, but he'll clearly see the visual benefit of GP lenses. Experiencing firsthand the power of vision from GPs is critical—not only for new wearers, but for soft lens wearers who have undergone challenges with their vision or with their ocular health. Empirical fitting allows you to provide the “Wow!”
There are several ways to empirically fit a GP lens. CLMA member laboratory consultants can provide helpful advice in tailoring the design. You can simply provide a patient's keratometry (K) or simulated K readings as well as refraction to the laboratory. Also, nomograms and calculators are available to help you solidify an initial design. One such tool is the GPLI Toric and Spherical Lens Calculator. It will suggest, depending on a patient's corneal toricity, a toric or a spherical design and recommend parameters. You can find this calculator and other helpful tools on the GPLI website at www.gpli.info (Table 1). Remember that even after empirical fitting, some minor changes to the design or power may be needed. However, it's quite common for the first empirically fitted design to result in the patient being able to adapt to lens wear.
Standard designs are becoming more common today than they were in the past. Custom designs with specified center thickness, peripheral curve radii and widths, optical zone diameters, and overall diameters are often unnecessary given the quality of designs we have available. In fact, fitting some GP lenses is now comparable to fitting soft lenses.
One essential aspect of fitting GP lenses is carefully assessing the lens-to-cornea fitting relationship with fluorescein, including both the central and peripheral fluorescein pattern. Use a Wratten filter to allow for best viewing. The optimal pattern shows very mild clearance throughout to the periphery with slightly greater clearance peripherally. Click N' Fit, one of the many resources available at www.gpli.info, provides an excellent overview of fluorescein patterns (Figure 1) and what occurs when you make changes to base curve radii and diameter.
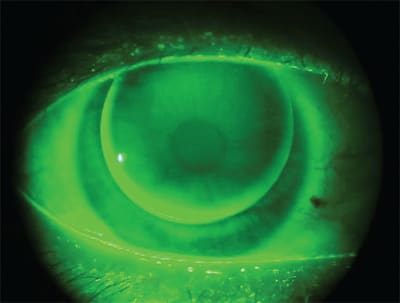
Figure 1. On-K base curve radius from Click N' Fit.
If there is excessive edge clearance, which results from a very flat and wide peripheral curve or from apical bearing, the patient could experience increased lens awareness due to lift off at the lens edge. The completeness of the blink may be compromised, resulting in increased potential for 3 o'clock and 9 o'clock staining or corneal desiccation. In this case, select a steeper peripheral curve radius and/or base curve radius. Conversely, insufficient edge clearance or edge seal-off causes poor tear exchange and inadequate lens movement, also often resulting in 3 o'clock and 9 o'clock staining. For insufficient edge clearance, flatten the peripheral curve radius.
If you choose to diagnostically fit your patient, use K readings as your guide for base curve selection. Most nomograms and calculators recommend a base curve radius that is flatter than K. For example, if your patient has K readings of 43.00 @ 180 and 44.00 @ 90, the initial base curve might be 42.75D. The base curve should be flatter than K because of the asphericity of the cornea—it flattens from the center to the periphery. To bracket for an alignment fit, select the base curve slightly flatter than K. After the lens is ordered and arrives, apply it to be sure that the fit exhibits optimum centration and desirable fluorescein pattern, then perform a spherical over-refraction.
If the first fitting rule is to choose a base curve slightly flatter than K, the second is to choose an ultrathin design if your patient has 1.50D or less of corneal astigmatism. Such a design reduces mass by 30 to 40 percent over a standard thickness design. Ultrathin designs produce lenses that are more likely to resist the effects of gravity and position on the eye such that optimum centration is achieved. If a lens continues to decenter inferiorly, apply a lenticular to the ultrathin design if the power dictates.
Remember that edge thickness is a key factor in lens centration and initial comfort. The ideal edge thickness is that of a –2.50D to –3.00D lens. If your patient requires a power ≥ –5.00D, a plus lenticular design is needed. All plus and low minus (<–1.50D) lenses should have a minus lenticular to increase the edge thickness.
With high astigmatic patients (>1.50D of corneal cylinder), a lens with a steeper-than-K base curve radius and/or a large optical zone will increase the risk of the lens flexing on the cornea and not correcting all of the patient's astigmatism. If the patient is experiencing reduced visual acuity, confirm flexure by performing keratometry over the lens. If there is no flexure, you'll obtain spherical readings. If you obtain toric readings over the lens, the lens is flexing. The first change would be to select a flatter base curve radius, then reduce the optical zone diameter. Refitting into a larger design with an increased optical zone diameter increases the sagittal depth and provides greater apical clearance.
It is important to always remember that when making a lens design change, make it a significant one. This would include changing the base curve radius by, at minimum, 0.50D, changing the overall diameter or optical zone diameter by at least 0.3mm, and changing the center thickness by 0.2mm (Szczotka, 2001). CLS
For references, please visit www.clspectrum.com/references.asp and click on document #191.

|
Dr. Bennett is assistant dean for Student Services and Alumni Relations at the University of Missouri-St. Louis College of Optometry and is executive director of the GP Lens Institute. You can reach him at ebennett@umsl.edu. |