


KERATOCONUS FITTING
Pearls for Fitting Keratoconus
Three practitioners share pearls from 30 years of clinical experience with fitting keratoconus patients.
| Dr. Phan graduated from the Pennsylvania College of Optometry and completed a one-year fellowship in cornea and contact lens at Jules Stein Eye Institute, UCLA. This fellowship was supported by an educational grant from The Vision Care Institute, a Johnson & Johnson company. She has joined the staff of optometrists at UCLA and is currently the contact lens specialist at Jules Stein Eye Institute. |
| Dr. Mondino has held the position of Chairman of the Department of Ophthalmology and Director of the Jules Stein Eye Institute since 1994. He is also a Bradley R. Straatsma Professor of Ophthalmology at the Jules Stein Eye Institute. |
| Dr. Weissman is a Fellow and Diplomate of the Cornea & Contact Lens Section, American Academy of Optometry and is currently serving as a Trustee for the California Optometric Association. He is a professor of Optometry, Southern California College of Optometry, Fullerton, Calif., and professor emeritus of Ophthalmology, Jules Stein Eye Institute, and Department of Ophthalmology, David Geffen School of Medicine at UCLA, Los Angeles. He has consulted for Vistakon, Alcon, Bausch + Lomb, and AMO. |
By Vivian Phan, OD; Bartly J. Mondino, MD; & Barry A. Weissman, OD, PhD, FAAO
Keratoconus is a non-inflammatory, bilateral but asymmetric, progressive steepening and thinning of the central cornea. Keratoconus primarily affects young adults and leads to visual difficulties and ocular discomfort (Krachmer et al, 1984; Zadnik et al, 1996; Rabinowitz, 1998).
Corneal GP contact lenses remain the primary visual management for keratoconus, but issues such as contact lens intolerance, chronic staining leading to scarring, and poor mechanical alignment can contribute to lens wear failures.
The following are clinical pearls derived from clinical experience in managing keratoconus patients at the Jules Stein Eye Institute at UCLA for 30 years, along with additional documentation by publications.
1. Cowboy Hat Philosophy
Many different clinical philosophies have been proposed on how to manage GP contact lens fitting for keratoconus. These include: flat (to flatten the corneal apex into a more normal shape), steep (to vault and thereby spare the corneal apex), and divided support (three-point touch) (Korb et al, 1982; Zadnik et al, 2005). The “cowboy hat” philosophy describes a design in which the contact lens is fit so that it is relatively steep in its “crown,” or central base curve, compared to the patient’s corneal apex to provide a light corneal apical touch, with a wide “brim” peripheral edge (Figure 1). A relatively steep base curve allows light apical clearance to spare the corneal apex from mechanical assault. The flat, wide periphery promotes adequate tear exchange and lens movement as well as better support in the periphery to take pressure off the apex of the cornea.
Increasing the width of the periphery also decreases the optic zone of the lens, which will minimize bubbles by decreasing the area of the tear meniscus. Satisfying these criteria can help minimize contact lens mechanical complications such as 3 o’clock and 9 o’clock staining, contact lens binding, and apical erosions (punctate epithelial erosions and epithelial defects). Epithelial defects have been found to occur more frequently in keratoconic eyes than in non-keratoconic corneas even in the presence of relatively steep GP lenses, and perhaps even in the absence of contact lens wear (Weissman et al, 1994).
To fit in the style of the cowboy hat philosophy, prescribe individually designed GP lenses or any of the named corneal GP keratoconic contact lens designs such as Rose K (Blanchard/Art Optical) or Dyna Cone (Lens Dynamics). These lenses range in overall diameter (OAD) from 8.0mm to 11.0mm.
2. Bigger is Better
Relatively larger intralimbal contact lenses such as Dyna Intra-Limbal (Lens Dynamics) or G.B.L. (Concise) can often improve centration, leading to a more optimized fit in moderate cones (Zhou et al, 2003; Barnette and Mannis, 2011). These lenses are slightly smaller than the corneal diameter (10.5mm to 12.0mm). Larger-diameter GP contact lenses have also been shown to enhance patient’s tolerance and adaptation—GP lenses become more comfortable when the upper lid does not rub over the superior edge during blinking (Mandell, 1988). Choosing a larger OAD is often helpful in refitting patients who present with a history of previous GP intolerance.
3. High Dk to Avoid Corneal Ring Clouding
Weissman (1994) documented three cases of corneal ring clouding observed in patients who had keratoconus. Given that most keratoconus patients are highly myopic, and that GP lenses have most of their thickness in the intermediate portion of the lens at the junction between the peripheral curve and the optical zone, Weissman proposed that this ring of corneal edema was analogous to previously described central corneal clouding. Central corneal clouding may be caused by a corneal surface that is never “uncovered by the contact lens optical zone,” (Korb and Exford, 1968). The three reported cases of ring edema were associated with GP lenses of relatively low Dk/t (less than 30 Fatt Dk units), whereas patients wearing GP lenses with moderate-to-high Dk/t values (greater than 60 Fatt Dk units) do not present as commonly with this complication.
A variety of new materials available in the market these days have made it easy to select high-Dk lenses for our patients. However, a similar clinical appearance has recently been noted in a GP scleral patient (Figure 2).
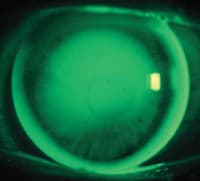
Figure 1. A well fit keratoconic eye with apical clearance, light inferior cone touch and wide peripheral edge.

Figure 2. Central ring clouding in a scleral GP lens patient.
4. Piggyback Lens Systems
Piggybacking with a soft lens can be a helpful clinical tool to help improve contact lens tolerance, defined by patient comfort as well as patient ability to wear the lenses without causing physiological harm to the cornea. Good examples of when to consider piggyback fitting include a keratoconic eye that is chronically abraded even with a steeply fit GP lens, chronic 3 o’clock and 9 o’clock staining, or scarring that cannot be otherwise treated. Because piggybacking introduces another lens or set of lenses into a patient’s care and cost, you should consider a piggyback lens system only when you are satisfied that the GP lens has an optimal mechanical fit.
In modern piggyback systems, a low-minus silicone hydrogel lens is typically placed beneath a well-fit GP. If there are issues with centration, a plus-powered soft lens can help center the GP. Keep in mind that the effective power of the soft lens under the rigid lens is expected to have about 20 percent of its original power (Woo and Weissman, 2011), and using a plus-powered soft lens may necessitate a refitting of the GP for mechanical as well as for optical reasons.
Weissman and Ye (2006) calculated that as long as both the rigid and soft lenses have been manufactured from moderate- to high-Dk materials (each greater than about 60 Fatt Dk units), there should be adequate oxygen supply to the cornea under daily wear conditions. Although rare, associations have been found between keratoconus patients and deep neovascularization (Korb et al, 1982). A small number of patients may exhibit corneal neovascularization with piggyback lenses. Discontinue such patients from piggyback lens wear and consider alternative methods of treatment.
5. Scleral Lenses
The bigger-is-better philosophy can be extended to GP scleral lenses that range in OAD from 15mm to 24mm. Patients typically adapt quickly to scleral lenses because the lens completely vaults the cornea, resting on the surrounding sclera and thus eliminating movement or irritation that is often noticed upon blinking with corneal GPs. Scleral lenses are an essential tool in fitting advanced cones. They are also indicated in decentered cones, pellucid marginal degeneration, piggyback or hybrid lens failure, poor comfort with corneal GPs, and moderate-to-severe dry eyes (Barnette and Mannis, 2011; Ye et al, 2007). The ideal fit for a scleral lens is apical clearance over the cornea extending from limbus to limbus and an alignment relationship with the sclera. Too much clearance in the apical center, however, can cause bubbles, whereas peripheral curves that are too tight can cause scleral blanching, intolerance, and difficulty with lens removal.
6. Frequent and Close Monitoring
Because keratoconus patients have a higher risk of complications, close monitoring is essential in the maintenance of successful lens wear (Weissman et al, 1994). After the completion of initial fit, a keratoconus patient should be followed every four months to six months even if asymptomatic, depending on the severity and evolution of the disease and the general lens tolerance of the patient. Clinicians may find that care for keratoconus patients seems to drop off after the age of 60. In a study analyzing contact lens trends, it was found that the number of lens wearers in general decreases after the age of 60, whether or not they have keratoconus. It was also found, however, that keratoconus patients require twice the amount of clinical care than do non-keratoconus patients regardless of age (Yeung et al, 1998).
Conclusions
Contact lens care of keratoconus patients is often challenging, complex, and involved, requiring cost and time on the part of both practitioner and patient. However, contact lens wear can restore vision without the need for surgery throughout the lifetime of most keratoconus patients. With much advancement in both lens material and design science, it is hoped that even fewer patients who have this disease will need to face surgical intervention in the future. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #205.