


Prescribing for Astigmatism
Managing Scleral Lens Flexure

BY JARED JAYNES, OD, & TIMOTHY B. EDRINGTON, OD, MS, FAAO
Because scleral lenses completely vault the cornea and rest on the sclera, corneal toricity does not dictate lens flexure as it does with corneal GP lenses. Scleral toricity is the major factor in scleral lens flexure.
Scleral toricity resulting in uneven alignment of the peripheral curve system on the scleral conjunctiva may lead to flexure. For example, if peripheral lens bearing is prominently nasal-temporal, this may contribute to flexure, resulting in an increase in with-the-rule (WTR) over-refraction (OR) cylinder.
Center thickness remains an important element in scleral lens flexure. On occasion, flexure may persist regardless of the fit and lens center thickness. If lens thickness cannot be increased without compromising lens fit or the underlying corneal health, consider a toric peripheral curve system, a front-surface toric lens design, or prescribe overlay glasses to achieve the best possible vision and patient satisfaction.
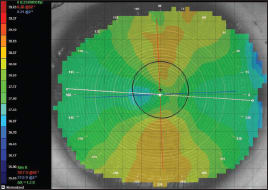
Figure 1. Right eye scleral lens over-topography. Center thickness of 0.25mm, flexure = 1.30D.
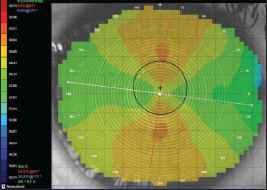
Figure 2. Right eye scleral lens over-topography. Center thickness of 0.32mm, flexure = 0.70D.
| Table 1 | ||||||
|---|---|---|---|---|---|---|
| How Changes in Lens Center Thickness Affect Scleral Lens Flexure | ||||||
| Trial #1 | Trial #2 | Trial #3 | Trial #1 | Trial #2 | Trial #3 | |
| OD | OD | OD | OS | OS | OS | |
| Lens center thickness | 0.16mm | 0.25mm | 0.32mm | 0.16mm | 0.25mm | 0.32mm |
| In situ visual acuity | 20/40 | 20/25-2 | 20/15 | 20/40+2 | 20/25 | 20/20 |
| OR residual cylinder | 2.25D WTR | 0.75D WTR | 0.50D WTR | 3.25D WTR | 0.75D WTR | 0.50D WTR |
| Measured on-eye flexure | 2.50D WTR | 1.30D WTR | 0.70D WTR | 2.75D WTR | 1.50D WTR | 1.10D WTR |
Case Report
An 18-year-old female soft toric lens wearer presented seeking an improvement in vision through her contact lenses. She is a collegiate softball player who desired relief from dust/debris accumulating behind her lenses. After discussing contact lens options, she was fit with 14.4mm-overalldiameter scleral lenses.
At the initial dispensing visit, the patient experienced reduced vision in both eyes due to residual WTR cylinder consistent with her scleral toricity. Topography over her scleral lenses identified flexure as being responsible for her decreased vision. Over the course of follow up, a series of thicker lenses reduced the visual complications of lens flexure (Figures 1 and 2, Table 1), and the patient reported excellent vision through the scleral lenses at her final visit. CLS
Dr. Jaynes, a graduate of Southern California College of Optometry (SCCO), is currently a cornea and contact lens resident at SCCO. Dr. Edrington is a professor at the Southern California College of Optometry. You can reach him at tedrington@scco.edu.