


LENS COMPLIANCE
Compliance Before, During and After Contact Lens Wear
Survey results shed new light on the top noncompliance behaviors, and practitioners offer tips on how to improve adherence to lens wear and care regimens.
By Sheila B. Hickson-Curran, BSc (Hons), MCOptom, FAAO
Patients who do not adhere to their prescribed regimens exist in all areas of health care. Studies have shown that about 35 percent of patients with glaucoma do not use their IOP-lowering drops as directed (Dietlein et al, 2005), 38 percent of patients with Type II diabetes fail to adhere to their insulin regimens (Cramer, 2004), and more than 40 percent of patients do not take their osteoporosis medicine (Boccuzzi et al, 2005). Failing to take medication for these diseases can have a significant impact on morbidity and mortality.
As we know, contact lens wearers often do not fully adhere to their practitioners' instructions on how to safely wear and care for their lenses. Fortunately, serious negative consequences such as microbial keratitis are unusual, but the rarity of serious complications may actually reinforce poor lens wear and care habits.
“Generally, I think patients want to do what is best. The intent to comply is there, if not always the execution,” says Susan Kovacich, OD, clinical associate professor at the Indiana University School of Optometry. “But when they begin to extend their wearing schedules or skip care steps without any negative consequences, patients become even more relaxed about proper lens care.”
Key Areas for Compliance
In a recently published paper, two colleagues and I summarized the evidence in the literature on a wide range of contact lens compliance steps and categorized them according to the degree of clinical importance associated with skipping or irregularly performing each step (Hickson-Curran et al, 2011). In the same paper, we reported the results of two online surveys to assess how well U.S. wearers of frequent replacement (not daily disposable) contact lenses adhere to common guidelines for healthy lens wear. To avoid biasing respondents to report better compliance than they actually practiced, the surveys were completed at home or other locations, and they were not in any way associated with eye care visits or eyecare practitioners' offices.
The first 645 contact lens wearers (ages 12 to 39), who were members of a consumer panel, were asked about lens replacement frequency. They may have also been asked about other products (e.g., cell phones, laundry detergent), so they were not aware the survey was sponsored by a contact lens company. A separate panel of 787 contact lens wearers (ages 18 to 39) was asked, again in an online survey, about a wide range of contact lens-related behaviors, including hygiene, cleaning practices and case replacement.
The results of both surveys, especially in the context of the literature on each topic, provide ample evidence that patients need to be educated continually.
Before: Hand Washing and Lens Replacement
Prior to contact lens wear, we want patients to wash and dry their hands, rinse the lenses correctly with solution (depending on modality and care regimen) and adhere to their replacement schedules.
Of these steps, poor hand washing is the most closely associated with an increased risk of infection (Radford et al, 2009). According to our survey, just a little more than half the respondents (56 percent) washed their hands with soap before handling lenses in the morning.
“This might seem like a basic hygiene step that we wouldn't need to mention, but we do,” says Arti Shah, OD, FAAO, a private practitioner in Santa Monica, Calif. “I emphasize washing with soap that is not cream-based and drying hands completely before handling lenses.”
Patients' compliance with lens replacement schedules has been a major topic of discussion among practitioners and contact lens manufacturers. Several studies suggest a relationship between modality and compliance (Dumbleton et al, 2010; Yeung et al, 2010), with most researchers agreeing that patients who wear daily disposable lenses exhibit the most compliant behaviors (Dumbleton et al, 2009). The simplicity of the daily disposable modality makes it easy to explain and remember.
Dumbleton and colleagues (2010) reported that compliance with a replacement schedule, regardless of modality, is associated with better comfort and vision at the end of the day and at the end of the wear cycle. Other research also suggests that comfort declines and unscheduled visits for clinical complaints, such as dryness, increase with longer periods of wear, even within the recommended replacement cycle (Hickson-Curran et al, 2010.
We do not have much data about the safety implications, if any, of various frequent-replacement modalities or of overwearing lenses beyond the recommended replacement schedule. Some recent studies that have attempted to make such connections have inherent weaknesses. If patients are not prospectively randomized to modality, the more frequent replacement groups are likely to contain a greater proportion of patients who were prescribed a shorter replacement cycle by their doctors specifically because those patients are compliance-challenged, prone to allergy or have already experienced an adverse event, hence biasing the sample.
The results of our lens replacement survey indicate generally low compliance with practitioners' recommendations on replacement frequency. I do not believe that modality “causes” noncompliance. Rather, compliance is a function of three factors: 1) how well patients understand the wear schedule; 2) their desire to comply; and 3) if they remember to make time in their busy lives to change their lenses on schedule.
Another factor, of course, is what instructions patients are given by their practitioners, and this isn't always well controlled. In one recent study, for example, 49 percent of the prescribing optometrists recommended a replacement schedule other than 2 weeks for patients wearing lenses the manufacturer recommended for 2-week wear (Dumbleton et al, 2010). This makes the question of compliance murkier, because a patient may be following his practitioner's instructions, but the practitioner has recommended a replacement frequency that differs from the lens manufacturer's recommendation.
“Trying to make patients happy by giving them a longer wear schedule than what the manufacturer recommends is not the answer,” says Dr. Kovacich. “All the clinical trials are performed with specific wear intervals based on the individual lens materials and wetting agents. It behooves us to recommend those same intervals, both for performance and consistency.” She finds that patients are much more likely to adhere to their lens replacement schedule when they have fresh lenses on hand. “That's why we strongly encourage every patient to purchase an annual supply of lenses,” she says. “When you break down the price for them, including rebates and insurance, most patients will agree that an annual supply is worthwhile financially, too.”
Smartphone-based applications and electronic reminder services are a great way to help tech-savvy patients remember when to replace their lenses, Dr. Shah says (see “Compliance Goes High Tech,” below), but for those who just can't seem to stay on track, she is quick to suggest daily disposable contact lenses.
| Compliance Goes High Tech |
|---|
| According to the Global Mobile Health Market report, 1.4 billion people will own smart phones by 2015—and about 500 million of them will be using health-related applications for their mobile devices. With all these computer-literate, smart phone-toting patients, practitioners should stay on top of the latest high-tech approaches to reminding them about contact lens replacement and office visits. Here are some options to consider: • Popular calendars, including Microsoft Outlook Calendar, Google Calendar and Apple's iCal, all allow users to establish recurring calendar appointments or tasks with reminders that pop up on the screen and sync to smart phones, too. • iTunes offers four contact lens reminder “apps” for the iPhone. BlackBerry and Droid each have a few, as well. Together, the app stores already boast a total of 17,000 mobile health applications. • Acuminder (www.acuminder.com) lets patients sign up for free text messages or e-mail reminders when it is time to change their lenses or schedule an appointment, regardless of the brand of lenses they wear. • LensAlert cases keep the reminder right where patients keep their lenses. • A video on YouTube highlights why patients need to clean their lenses and stay on their replacement schedule. To view, go to http://www.youtube.com/acuvue#p/c/5D2215A5200FDECF/0/0rEcXTNF1To. |
During: Overnight Wear and Water Exposure
The most important risk factor for microbial keratitis is overnight contact lens wear (prescribed or not). Epidemiological studies have shown the rate of microbial keratitis with overnight wear of soft contact lenses has remained steady at 4 to 10 times the rate of microbial keratitis with daily wear (Schein et al, 2005; Stapleton et al, 2009; Schein et al, 1989). Overnight wear is also associated with higher rates of corneal infiltrates (Stapleton et al, 2007; Szczotka-Flynn and Diaz, 2007).
When warning her patients about sleeping in their lenses, Dr. Shah focuses on the eye's need for oxygen. “That gives me an opportunity to talk about the benefits of silicone hydrogel materials, as well as the importance of having spectacles in addition to contact lenses,” she says. “Not having functional eye-glasses can be a major contributor to noncompliance. When patients can't read without their lenses, they are most likely going to fall asleep in them.”
Contact with water is another major concern during contact lens wear. In one study, 96 percent of lenses worn for 30 minutes of swimming were contaminated with pathogens, compared to only 19 percent of those not worn during swimming (Choo et al, 2005). Wearing goggles appears to reduce but not eliminate the bacteria adhering to lenses (Wu et al, 2011).
Although clinicians instruct patients how to apply, remove and clean their contact lenses, Dr. Shah says the missing piece is what not to do while wearing their lenses.
“When I tell patients that I don't want them to swim in lakes or pools, engage in water sports, use a hot tub or shower while wearing their lenses, they are very surprised, because they have never heard that before,” Dr. Shah says. “I tell them it's just not worth the risk of getting an infection that might keep them out of contact lenses and will certainly cost a lot of time and money to take care of.”
After: Cases and Cleaning
Considering current patterns of contact lens case cleaning, exposure to tap water is highly likely. More than half our survey respondents (53 percent) reported that they rinse their cases with warm or hot tap water, and 19 percent said they rinse with cold water (Table 1).
| LENS CASE CLEANING METHOD INVOLVING CERTAIN OR POSSIBLE EXPOSURE TO TAP WATER | (N=787) |
| Rinse lens case with warm or hot tap water | 53% |
| Wash lens case with soap | 20% |
| Rinse lens case with cold tap water | 19% |
“Patients really don't perceive their tap water as ‘dirty,’” Dr. Kovacich says. “After all, they drink it and bathe in it. When we say, ‘rinse your case,’ they assume we mean with water. We need to be very clear and specific about the fact that tap water should never come into contact with soft contact lenses.”
Of even greater concern than how patients clean their cases is the finding that many rarely if ever clean them. Only 26 percent of respondents to our survey reported cleaning the case daily. The median was 2 to 3 times per week, which may not be unreasonable, but one in three respondents clean the case monthly or even less often (Figure 1).
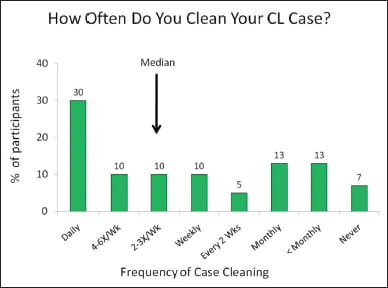
Figure 1. Survey results of how often patients clean lens cases.
The ideal interval for case replacement is unknown. The FDA recommends replacement every 3 to 6 months, and some practitioners advise replacement every 1 to 3 months. About 40 percent of the people we surveyed said they use a lens case for a full year or longer.
“Topping off” or failing to completely empty and replace the contact lens disinfecting solution in the case is a common practice that was linked to the Fusarium keratitis outbreak a few years ago (Chang et al, 2006; Levy, 2007). Less than half the respondents in our survey (46 percent) said they fill the lens case with solution every evening, meaning that the other half performs this necessary step irregularly.
Rubbing lenses is another aspect of the cleaning regimen that is often ignored. Although the literature is quite clear that rubbing helps to remove the microbial load on the lenses (Kilvington and Lonnen, 2009; Buck et al, 2000) and may play an important role in preventing microbial keratitis (Ahearn et al, 2008; Butcko et al, 2007), the “no rub” language on many multipurpose solution labels has left many patients understandably confused. The majority of our survey respondents (75 percent to 77 percent) omit this step.
Dr. Kovacich finds it important to share with her patients new data on the benefits of rubbing contact lenses while cleaning them. “I always try to give them some facts to support what I'm recommending. It makes the instructions more memorable, and it helps to counteract that natural human tendency to skip steps.”
Making a Difference
Solving the compliance puzzle requires that we first understand the reasons for poor compliance, which can be grouped into three general categories: 1) Patients who do not understand instructions; 2) Patients who ignore instructions, believing “nothing bad will happen”; and 3) Patients who forget or procrastinate. Each of these reasons requires a different approach.
When patients don't understand the clinician's instructions (or the reason for them), more education is needed. Dr. Shah says the data suggest she needs to redouble her efforts with established contact lens wearers who may have accumulated bad advice and developed bad habits over the years. “The toughest cases are the patients who feel comfortable and see fine, even though they don't adhere to my instructions,” she says. “Sometimes the best approach is to just start over with a new lens, a shorter wearing schedule, a new solution, new eye drops and new instructions for care.”
What should you do when a patient ignores your instructions because he believes nothing bad will happen? One of Dr. Shah's patients, a 45-year-old man who had been sleeping in conventional hydrogel lenses for 2 to 3 weeks at a time, was skeptical about needing to change. “What turned it around was when I told him he had some corneal edema, and a change in his prescription after 1 week of daily wear proved me right,” she says. “That seemed to validate the message for this patient.”
It may be that certain types of patients are simply more likely to be noncompliant. My co-author in the recent study on compliance, Robin Chalmers, OD, FAAO, an Atlanta-based clinical trial consultant, has been investigating safety and compliance patterns by age as co-chair of the Contact Lens Assessment in Youth (CLAY) team.
“We are finding that the youngest contact lens wearers (ages 8 to 15 years) are likely very compliant,” Dr. Chalmers says. “They are under their parents' guidance, have access to care, and they seem to be wearing lenses appropriately.” In the 16- to 25-year olds, however, she has seen a higher rate of corneal infiltrates and other events that interrupt contact lens wear. She suggests that practitioners might want to rethink how they prescribe for this age group. “Rather than looking for the cheapest option for that freshman in college, they might want to consider daily disposable lenses for this compliance-challenged and higher-risk group.”
Finally, busy lives, procrastination and forgetfulness are all major factors in contact lens noncompliance. Just as we don't all floss our teeth or exercise as often as we should, patients lose track of dates and forget to carry out key steps in the care regimen. If practitioners focus on changing the behaviors with the greatest clinical impact and providing convenient reminder tools, they can help bring patients closer to full compliance. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #194.
Dr. Kovacich is a consultant for Ciba Vision. Dr. Shah is a professional affairs consultant for Vistakon and Clinical Research Optometrist for AcuFocus. Dr. Chalmers is a clinical trial consultant with consulting relationships with Alcon Research Ltd., Bausch + Lomb, Ciba, Johnson & Johnson Vision Care and Inspire Pharmaceuticals.

|
Sheila Hickson-Curran is director of Medical Affairs for Vistakon, Division of Johnson & Johnson Vision Care Inc. |