


Refractive Focus
Dry Eye Disease and Visual Performance

By David A. Berntsen, OD, PHD, FAAO
With this issue of Contact Lens Spectrum focusing on dry eye and ocular surface disease, now is a great time to review what is currently known about visual performance in patients who have dry eye.
In addition to the typical physical symptoms that dry eye patients experience (e.g., burning, stinging, pain, scratchiness, redness, etc.), they also experience blurred vision. The blurred vision that dry eye patients experience in the early stages of the disease is often transient in nature and temporarily corrected with blinking, making it difficult to detect with standard clinical tests. In later stages of the disease process, visual disturbance is more substantial and consistent.
Stages of Visual Disturbance
In the earlier stages of dry eye disease, visual fluctuations occur secondary to instability of the tear film and rapid tear film breakup time (TFBUT) between blinks (Figure 1). Rapid TFBUT leads to reduced contrast sensitivity, especially at high spatial frequencies (Ridder et al, 2005). Visual fluctuations follow a diurnal pattern and increase later in the day (Begley et al, 2003), when increased fluctuations are associated with shorter intervals between blinks and longer reading times (Walker et al, 2010). Tasks that tend to decrease blink rate (e.g., computer use, reading, etc.) exacerbate these fluctuations.
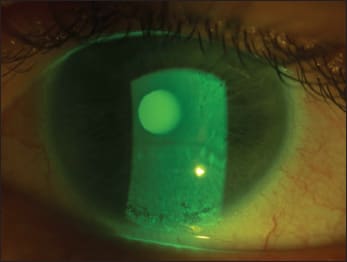
Figure 1. Tear film breakup, which results in visual fluctuations between blinks.
In contact lens patients, breakup of the tear film on the anterior surface of the contact lens leads to visual fluctuations. Visual performance improves in these contact lens wearers when they use artificial tears (Thai et al, 2002; Ridder et al, 2005).
Because blinking momentarily re-establishes the tear film, these visual disturbances are not easily detected using standard Snellen or logMAR visual acuity testing; patients simply read the acuity chart at the moment after a blink when vision is the clearest. To detect the visual disturbances experienced by these patients in the earlier stages of dry eye disease, a test must be able to evaluate visual performance at discrete time points after a blink.
In chronic, more severe stages of dry eye disease, corneal surface damage (such as epithelial damage and staining) results in chronic reductions in visual acuity and contrast sensitivity (Figure 2). In severe cases, reductions can be more easily measured with standard clinical techniques because blinking does not meaningfully improve vision.
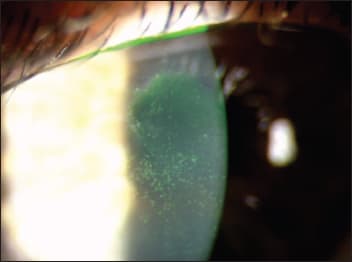
Figure 2. Central corneal staining leads to reduced visual performance that is not typically corrected by a blink.
Measuring Visual Disturbance
An issue in dry eye disease is the poor association between patient symptoms and objective dry eye tests (Nichols et al, 2004); because of this, patient symptoms are typically weighed more heavily in a dry eye diagnosis compared to clinical testing (Begley et al, 2003). Measuring visual disturbances in dry eye disease (both with and without contact lens wear) is no exception to this issue. Given that transient fluctuations in vision are not detectible by standard clinical techniques, let's look at what methods are currently being used to measure these disturbances.
Multiple tests to assess visual performance have been described in the literature; however, there is currently no single, accepted clinical test available to measure visual performance in dry eye disease patients. (For a recent review of impaired visual performance and testing in patients who have dry eye, see Ridder et al, 2011.)
Functional visual acuity (FVA) tests have been used to capture the decay in vision between blinks. FVA was first described 10 years ago. The instrument utilized a Landolt C of various sizes and orientations to determine visual acuity during sustained openeye periods. This technique can detect the decrease in visual acuity in dry eye patients that is associated with activities that have an increased inter-blink period such as reading and computer use (Kaido et al, 2007).
Sequential aberrometry measurements have also been used to measure the degradation in optical quality associated with dry eye disease. As the tear film breaks up, distortions in the spot pattern of a Shack-Hartmann aberrometer are evident (Figure 3). These distortions result in measurable increases in higher-order aberrations (HOAs) of the eye, which in turn decrease retinal image quality and contrast sensitivity (Liu et al, 2010).
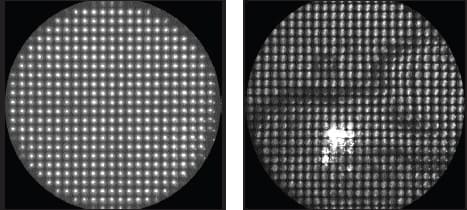
Figure 3. Aberrometry images showing a normal image (left) and a distorted image (right) due to tear film disruption. (Images obtained with the assistance of Jason Marsack, PhD.)
Along these same lines, corneal surface indices that quantify surface regularity have been utilized with corneal video keratography systems. This technique has been used to detect tear film instability in dry eye patients compared to normal patients (Liu and Pflugfelder, 1999).
Techniques that utilize interference patterns obtained as changes occur in the thickness of thin films can also be utilized to measure tear film thickness. Such methods have been used to demonstrate that artificial tears can increase tear film stability, increase lipid layer thickness, and decrease the rate of tear film thinning (King-Smith et al, 2010; Korb et al, 2005).
Definitive Test a Goal
The field has come a long way in being able to detect visual disturbances in dry eye patients. Methods now exist that can measure differences in visual performance between dry eye and normal patients. Though there is not a single, quick, clinically accepted test available to detect visual performance issues in dry eye patients, Ridder et al (2011) noted that previous research has identified the parameters needed to develop such a test. We can look forward to the day when a validated, easy-to-use clinical test is commercially available. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #200.
| Dr. Berntsen is an assistant professor at the University of Houston College of Optometry. He is also a consultant to B+L. |