


Contact Lens Case Reports
Cloudy Vision With Sclerals


By Patrick J. Caroline, FAAO, & Mark P. André, FAAO
We hear it all too frequently from our scleral lens patients—the need to remove their lenses every two to four hours due to a “cloudy” or “foggy” opaque substance that accumulates beneath their lenses (Figure 1). The condition can be bilateral but is often reported to be significantly worse in one eye than in the other. Patients quickly learn that they can resolve it by removing the lens, rinsing the lens surfaces with preservative-free saline, replenishing the bowl with fresh saline, and reapplying the lens. Patients then often reports good vision for another two to four hours. For some patients, this is the numberone complication that they experience with this lens type.
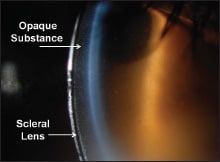
Figure 1. Opaque substance in the tear reservoir of a scleral lens.
Seven Clinical Findings
Following are a few clinical impressions that we've noted about this condition.
1. How often does this “cloudy/foggy” substance occur in patients wearing scleral lenses? We would estimate that the condition occurs (in varying degrees) in approximately 1 in 5 patients.
2. Does the condition improve with time? For some patients, the answer is yes. There is no doubt that in some individuals, the first month of lens wear is the worst, after which the frequency of the required lens removal and reapplication becomes less. In others, the condition must be managed through modifications of the existing contact lens parameters.
3. Does it ever go away on its own? The answer in our experience is no. While some patients experience a type of adaptation and lessening of the clouding/fogging, it rarely, if ever, disappears completely on its own.
4. Is the condition associated with any deposits or non-wetting of the lens surfaces? The answer here is no. The lens surfaces are frequently free of any deposits or non-wetting. Following lens removal, the opaque substance seems to be completely removed with a simple saline rinse of the posterior lens surface.
5. Is the condition associated with any underlying corneal edema? The answer is usually no, it is not. In most patients, the underlying cornea is free of any corneal edema. However, the clouding does need to be differentiated from true corneal clouding that has occurred in some patients in which their underlying condition has resulted in a compromised endothelium. In these patients, endothelial cell counts may have decreased to a critically low level, i.e., less than 500 cells per square millimeter, and in this situation the subjective cloudy or foggy vision may indeed be secondary to hypoxia.
6. What is it? To date no one appears to know the exact nature of the opaque substance. Our working hypothesis is that it is perhaps an accumulation of mucin-rich tears related to excessive pressure of the haptic on the mucin-rich goblet cells of the bulbar conjunctiva and/or excessive interaction of the lens edge on the palpebral conjunctiva. When this is combined with a greater-than-normal vaulting (in excess of 400 microns), the volume of the fluid interface is great enough to dramatically affect the patient's visual acuity.
7. Is there anything that can be done to lessen the formation/accumulation of the opaque substance? The answer is yes. Clinical experience has taught us that the condition can be lessened in two ways: by redesigning the haptic or scleral landing zone of the lens to create less interaction with the bulbar and palpebral conjunctiva and by avoiding central lens vaulting in excess of 400 microns. CLS
| Patrick Caroline is an associate professor of optometry at Pacific University. He is also a consultant to Paragon Vision Sciences. Mark André is an associate professor of optometry at Pacific University. He is also a consultant for CooperVision. |