


GP Insights
Do We Need Fenestrations for Scleral Contact Lenses?

By Gregory W. Denaeyer, OD, FAAO
Fenestrations are 1mm holes that are sometimes drilled into scleral contact lenses. You may be wondering why fenestrations were first invented and what their purpose is. Let's look at the history behind the use of fenestrations and whether their use is still applicable for today's scleral lenses.
Historical Use of Fenestrations
Before the development of hyper-Dk GP materials, scleral contact lenses were first made from PMMA and then eventually from low-Dk GP materials. Many patients wearing these early prototypes developed significant corneal edema secondary to insufficient oxygen permeability from the low-Dk materials and due to the slow tear exchange that is inherent to scleral lens function. In addition, scleral lenses generally have reduced oxygen permeability regardless of material as they are often manufactured three to four times thicker than corneal GP contact lenses are to avoid on-eye flexure. Fenestrations within the optic zone of scleral lenses have historically been used for air ventilation to overcome these oxygen deficits.
However, the development of GP material polymers that have Dk values of 100 or more has virtually eradicated complications from hypoxia, making fenestrations no longer necessary for air ventilation.
Indications Today
The use of fenestrations persists for corneal-scleral (12.5mm to 15mm) or mini-scleral (15mm to 18mm) contact lenses. The primary reason for utilizing fenestrations for these lens types is to reduce negative pressure beneath the lens, which allows for less on-eye suction and easier lens removal. It is also believed that a fenestration will allow for enhanced reservoir exchange. Finally, in cases in which bubbles form because of insufficient reservoir capacity, a fenestration may reduce a bubble or allow it to completely escape.
Complications
One possible complication of fenestrations is that they may allow scleral lenses to settle into the eye, which would decrease their vaulting capability. This may cause a lens that would normally provide adequate clearance to exhibit some corneal bearing.
I mentioned earlier that fenestrations may help reduce or eliminate bubbles, but fenestrations may also create bubbles. Sometimes these bubbles are small and of no consequence to the fit, vision, or health of the patient. However, large bubbles can significantly reduce negative pressure, which negatively affects the scleral lens fit by eliminating the semi-seal and allowing the lens to move (Figure 1). Larger bubbles may also negatively affect vision if they migrate over the patient's visual axis. Persistent bubbles that routinely reside in the same area can lead to tissue desiccation.
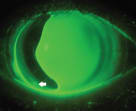
Figure 1. A large bubble in a mini-scleral lens formed secondary to a fenestration (arrow).
The Verdict
The advent of hyper-Dk GP materials has eliminated the need to fenestrate the optic zone to create air-ventilated scleral lenses. For most cases, a well designed corneal-scleral or mini-scleral lens will function best without a fenestration. In fact, in many cases a fenestration will create complications that wouldn't have existed otherwise. CLS
| Dr. DeNaeyer is the clinical director for Arena Eye Surgeons in Columbus, Ohio, and a consultant to Visionary Optics, B+L, and Aciont. You can contact him at gdenaeyer@arenaeyesurgeons.com. |