


POSTSURGICAL GP FITTING
Multifocal GP Lenses for Postsurgical Eyes
Despite significant advances in ocular surgery, some presbyopic patients require additional correction. GP lenses address a multitude of needs.
By Douglas P. Benoit, OD, FAAO

|
Dr. Benoit practices in a multi-subspecialty ophthalmology group in Concord, N.H. He is a Diplomate and currently Chair of the American Academy of Optometry Section on Cornea, Contact Lenses and Refractive Technologies. |
Advances in healthcare technology have made it possible to treat disease, repair problems, and replace organs, giving us longer, healthier lives. In eye care, cataract surgery has rocketed forward with the development of intraocular lenses (IOLs), including implants that can correct astigmatism and presbyopia, and advances in surgical techniques that facilitate rapid recoveries and allow procedures to be performed in an outpatient setting.
Tremendous strides have also been made in corneal transplantation surgery, allowing patients who have endothelial breakdown, central scarring, or advanced keratoconus to experience clearer vision and to have a better quality of life. In addition, refractive procedures have progressed well beyond radial keratotomy to include photorefractive keratectomy, laser in-situ keratomileusis (LASIK), phakic IOLs, and clear-lens extractions. All of these surgical interventions have evolved to the point where combining procedures is now commonplace.
Despite these advances, however, a small number of patients are left with less-than-optimal results (Steele, 2007). Even the use of LASIK to address residual refractive error after penetrating keratoplasty (Hardten, 2004) or IOL implantation (Pinero, 2010) does not correct vision 100 percent. For the best visual acuity after these procedures, we often turn to contact lenses.
Soft lenses may be successful in some cases, but frequently, the best physiological and visual results can be obtained only with a GP design (Szczotka-Flynn, 2003). Fortunately, we have a wide array of GP lens materials and designs at our disposal, making it possible to restore vision to near normal levels for most of these patients. The following cases are just a few examples of the numerous possibilities.
Case #1: GPs After LASIK and IOL Implantation
A 66-year-old man was 11 years post-LASIK and two years post-bilateral extracapsular cataract extraction (ECCE) with posterior chamber (PC) IOL implantation. He was interested in wearing contact lenses to free him from reading glasses. The patient had dry eyes for which he used cyclosporine ophthalmic emulsion 0.05% (Restasis, Allergan) twice daily. His ocular and general health was otherwise unremarkable.
Manifest refraction was OD +0.50 –1.00 x 010; OS +0.25 –1.25 x 180; 2.25D add OD and OS. Vision with this correction was 20/20 OD, OS, and OU at distance and near. Anterior segment evaluation was positive for meibomian gland dysfunction (MGD) OD and OS, arcus senilus and LASIK flap scars OD and OS, and PC IOL with clear capsules OD and OS. Keratometry readings were OD 42.50/44.50 @ 90; OS 43.00/45.12 @ 90 with clear, regular mires OD and OS.
Based on these K readings, I chose a biaspheric multifocal GP design in Boston XO (Bausch + Lomb [B+L]) material and ordered the following:
• OD: 7.75mm base curve radius (BCR), plano power, 9.5mm overall lens diameter (OAD), 2.50D add in a 3.0mm zone.
• OS: 7.75mm BCR, –0.25D power, 9.5mm OAD, 2.50D add in a 3.0mm zone.
At dispensing, the patient's distance vision was 20/20 OD, OS, and OU, and near vision was 20/25 OD, OS, and OU. Both lenses had a superior-central position with good movement in all positions of gaze. Fluorescein patterns showed slight apical clearance and good peripheral clearance. My staff taught the patient proper lens application and removal techniques and reviewed and demonstrated lens care with Boston Simplus Multi-Action Solution (B+L). I instructed the patient to gradually build up his wearing time and to return in one week.
At the one-week progress evaluation, the patient said his distance vision was good, but he felt his near vision could be improved. He also noted some discomfort with the right lens. Visual acuity was 20/20 OD, OS, and OU at distance and 20/30 OD, OS, and OU at near. An over-refraction of +0.75D OD and OS at near brought the vision to 20/20. Slit lamp biomicroscopy showed clean lenses. Each lens had a slight lid attachment, both were positioned superior-centrally, and movement was good in all gaze positions. Fluorescein evaluation again showed slight apical clearance OD and OS with good peripheral clearance OS but marginal peripheral clearance OD. I decided to flatten the BCR OD to increase peripheral clearance, and I increased the add power to 3.25D OD and OS. I ordered the following:
• OD: 7.80mm BCR, +0.25D power, 9.5mm OAD, 3.25D add in a 3.0mm zone.
• OS: 7.75mm BCR, –0.25D power, 9.5mm OAD, 3.25D add in a 3.0mm zone.
The resultant lenses provided 20/20 vision OD, OS, and OU at distance and near, with optimal fit and comfort. The patient is happy with his decision to enhance his vision with multifocal GP lenses.
Case #2: Post-LASIK
A 57-year-old man, 12 years post-bilateral LASIK, presented for a comprehensive eye examination. He had been wearing GP lenses to correct his residual refractive error but had recently lost one lens and was wearing spectacles. He was interested in multifocal contact lenses. He said he experienced spectacle blur lasting more than two hours after removing his previous GP lenses. Except for hypercholesterolemia, for which he was taking a statin drug, his general health was unremarkable.
Vision with his current spectacles at distance and near was 20/20-2 OD and 20/25 OS. Manifest refraction was OD –2.25 –1.00 x 083; OS –1.75 –1.25 x 163; 1.75D add OD and OS. Vision with this prescription was 20/20 OD, OS, and OU at distance and near. Anterior segment slit lamp evaluation showed MGD, arcus senilus, Hudson-Stahli line, Vogt's limbal girdle, and LASIK flap scars OD and OS. Keratometry revealed flat corneal curvatures of OD 39.37/38.50 @ 075; OS 38.25/38.50 @ 150. The mires had a slight blur OD and OS.
These flat keratometry readings indicated the need for a reverse geometry back surface lens to establish a comfortable, healthy lens-to-cornea fitting relationship. Once the back-surface fitting characteristics were established, a front-surface multifocal design was added to achieve optimum vision at all distances. The final lenses incorporated a reverse geometry back surface/biaspheric multifocal front-surface design in Boston XO material, with OD and OS base curve radii/fitting curves of 8.44mm/7.67mm and lens diameter of 10.5mm. Powers were –5.75D OD and –6.50D OS, with 2.00D add OD and OS in a 4.0mm zone.
The patient's visual acuity was 20/20-1 OD and 20/25+2 OS at distance and near. Both lenses had a central fit in primary gaze and 1mm of movement with the blink in all positions of gaze. Fluorescein evaluation showed mild apical pooling, good midperipheral alignment and good peripheral clearance OD and OS. My staff taught the patient proper cleaning technique using Optimum Cleaning Solutions (Lobob Laboratories Inc.).
At the progress evaluation two weeks later, the patient's visual acuity was the same as at the previous visit. He reported good comfort and no spectacle blur upon lens removal, even after 14 hours of wear. The fit, movement, and fluorescein patterns remained the same, with no superficial punctate keratopathy in either eye.
Case #3: Keratoconus and Post-IOL Implantation
A 65-year-old woman was referred by a cornea surgeon for a contact lens evaluation. The patient has keratoconus and had recently undergone ECCE with PC IOL implantation. She did not want to wear eyeglasses. Her general health was remarkable for mild hypertension and hypercholesterolemia, both of which were controlled by medication and exercise.
Uncorrected visual acuity was 20/125 OD and 20/25-2 OS at distance. Manifest refraction was OD +1.50 –1.75 x 038; OS +0.50 –0.25 x 105; 2.50D add OD and OS. Vision with this correction was 20/40 OD and 20/20 OS at distance and near. Biomicroscopy revealed moderate MGD, pinguecula on the bulbar conjunctiva, and Fleischer's ring and Vogt's striae OD and OS (Figure 1). Both IOLs appeared well positioned, and the capsules were clear. Keratometry revealed moderate distortion OD, mild distortion OS and the following curvatures: OD 45.25/46.50 @ 060; OS 41.50/44.00 @ 095. These values were in contrast to the simulated keratometry values obtained with corneal topography (Figure 2). This is a good example of why both keratometry and corneal topography are helpful when fitting a patient who has irregular corneas.
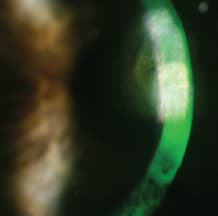
Figure 1. Right eye of patient from Case #3, showing scarring from keratoconus.
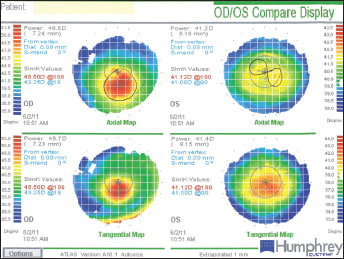
Figure 2. Topography maps of patient from Case #3.
I chose a biaspheric multifocal GP design for this patient. Based on the manufacturer's fitting nomogram, I ordered the following:
• OD: 7.35mm BCR, +1.00D power, 9.5mm OAD, 2.50D add in a 3.0mm zone.
• OS: 7.95mm BCR, plano power, 9.5mm OAD, 2.50D add in a 3.0mm zone.
Distance vision with these lenses was 20/40 OD and 20/25 OS. Near vision was 20/40 OD and OS. A distance over-refraction of –0.50D OD improved vision to 20/25, while a –0.25D change OS improved vision to 20/20. At near, an over-refraction of +0.75D OD and OS improved acuity to 20/25 OD and 20/20 OS. At the slit lamp, both lenses had a central to inferior-central position in primary gaze. Movement of both lenses was adequate in primary gaze, but translation was poor on downgaze. Fluorescein evaluation revealed slight apical clearance OD and OS, but poor peripheral clearance.
I ordered new lenses in the following parameters:
• OD: 7.40mm BCR, +0.75D power, 9.8mm OAD, 3.00D add in a 3.0mm zone.
• OS: 8.05mm BCR, +0.25D power, 9.8mm OAD, 3.00D add in a 3.0mm zone.
Comfort and vision improved with these lenses. Visual acuity was 20/25 OD and 20/20 OS at distance and near. Both lenses had a more superior-central fit in primary gaze and translated well when the patient looked down to read. Fluorescein evaluation showed slight apical clearance and good peripheral clearance in both eyes (Figure 3). At the most recent follow-up visit, the patient was happy with her lenses and liked the visual freedom that they provided.

Figure 3. Contact lens fit on right eye of Patient in Case #3.
Custom Designs for Complex Cases
These cases illustrate the relatively straightforward approach for fitting GP lenses to postsurgical eyes. Thanks to new technology, GP laboratories can produce truly custom designs for complex cases. In Case #2, for example, the fitting curve was significantly steeper compared to the central curve, which provided a great fit and very good vision. Years ago, when design choices were more limited, a good physiological fit might have compromised the patient's vision. But with today's improved technology, I was able to design a contact lens incorporating a multifocal front surface for excellent visual acuity while ensuring long-term corneal health.
That said, it is important in these cases to place a contact lens on the eye and evaluate the fit. You can better assess the physical fit, comfort, and vision with a diagnostic fitting, and subtle changes that will ensure success can be seen firsthand. Assessing the lens on the eye also reinforces the value of the entire fitting process for the patient.
Readily Available
As these cases show us, even patients who have good vision after surgery may still want better vision, and the desire to not need eyeglasses is often a strong motivator. In each of these cases, the best contact lens was a GP multifocal that was designed with relative ease to meet the physiological requirements of the cornea and achieve the visual result that each patient wanted.
The lenses used for these patients are not unique to one laboratory. The multitude of laboratories that are members of the Contact Lens Manufacturers Association are all capable of producing custom lenses for almost any patient's need. Corneal lenses, minisclerals, sclerals, toric/bitoric lenses, bifocal/multifocal lenses, and essentially any combination of these designs is possible. Investigate the laboratories in your area, talk to their consultants, and embrace the freedom that GP contact lenses can provide. CLS