


CONTACT LENS ADVANCES
Advances in Contact Lens Practice
Innovations in designs and materials have given practitioners new tools for more successful lens fitting.
By Barry A. Weissman, OD, PhD

|
Dr. Weissman is a Fellow and Diplomate of the Cornea & Contact Lens Section, American Academy of Optometry and is currently serving as a Trustee for the California Optometric Association. He is a professor of Ophthalmology, Jules Stein Eye Institute, and Department of Ophthalmology, David Geffen School of Medicine at UCLA, Los Angeles, and adjunct professor of Optometry, Southern California College of Optometry, Fullerton, Calif. He has consulted for Vistakon, Alcon, Bausch + Lomb, and AMO. |
Contact lens practice has evolved dramatically over this clinician's active career of four decades. It has developed from a purely commercial enterprise, with lenses manufactured in garages and sold to naïve patients by almost equally naïve clinicians who understood some optics and some mechanics but little of physiology, immunology, or microbiology, to a set of sciences driven by evidence-based medicine.
Advances in the pipeline should in the next few decades produce devices that will correct vision, perhaps some that will decrease or reverse myopia, while having little impact if any on the tissues over which they ride.
Advances in GP Sclerals
Although we have had notable improvements in GP lens materials and lens design over the past few decades, arguably the most important advance is in the resurgence of GP sclerals.
The original practical contact lenses, introduced in Europe more than a century ago, were large glass shells covering the entire front of the eye. Eventually called “sclerals” or “haptics”—as opposed to the later and smaller corneal rigid or semi-scleral hydrogels—because they do not touch the cornea but rather align with, and rest upon, the less sensitive sclera, this lens design has undergone a recent resurgence. Led by “pioneers” Drs. Don Ezekiel, Perry Rosenthal, and Rob Breece, scleral lenses, now made from high-tech oxygen permeable plastics, have shown an ability to serve a previously underserved—but admittedly small in numbers—group of desperate patients who suffer from various eye disease states. These include patients who have severe corneal irregularity (Figure 1) due to advanced keratoconus, trauma, and post-corneal graft (patients for whom more normal corneal designs fail for a variety of causes), but primarily those who have severe dry eye due to diseases such as ocular cicatricial pemphigoid, Stevens-Johnson syndrome, and graft versus host disease (secondary to treated lymphoma, etc.).
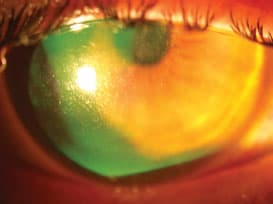
Figure 1. Keratoglobus eye wearing custom GP scleral lens.
Scleral lenses were first made from glass and then, after World War II, from polymethylmethacrylate (PMMA). They were abandoned for the most part in the 1950s in favor of corneal PMMA lenses and then later in favor of GPs and the popular hydrogels invented by Professor Otto Wichterle. These newer designs offered good vision correction and enhanced ocular tolerance, the former through tear exchange, the latter through size and flexibility, for the cosmetically driven, primarily mildly and modestly myopic populations.
The gradual enhancement of contact lens plastic oxygen permeability (Dk) over the succeeding decades, in both rigid and flexible formats, eventually resulted in our pantheon of modern GP and soft materials, all but eliminating hypoxia during daily wear as a clinical issue. Parallel advances in understanding lens design and optics extended the prescriptions addressable to patients who have significant astigmatism, presbyopia, and those suffering the extremes of optical correction, both myopic and hypermetropic/aphakic.
The anecdotal story is that about a decade ago, Donald Ezekiel of Perth, Australia, was the first to have the epiphany that the time had come to revisit the scleral lens, now made in a high-Dk material. He petitioned for the availability of large-diameter rigid lens buttons, and this led to the development of several clinical centers providing such lenses in Boston, London, and Perth. A cadre of devoted clinicians developed by experience the rules that we are now learning to help these patients (van der Worp, 2010), followed by the development of several manufacturing laboratories providing these large-overall-diameter (16mm to 25mm) high quality lenses.
The primary clinical goal of current GP scleral lens application is to arrive at a lens that totally vaults the patient's corneal surface, limbus to limbus. Any significant corneal touch will likely result in corneal irritation and erosion as well as other secondary concerns such as intolerance.
The secondary clinical goal is to provide a scleral portion (or haptic) that neither overly compresses the conjunctiva (resulting in large areas of conjunctival vascular blanching) nor is so loose as to allow free enough exchange of fluids to generate bubbles under the lens corneal vault. Such bubbles, if immobile, will likely desiccate the underlying corneal epithelium, again leading to corneal erosion with its secondary consequences.
The third clinical goal is to provide the necessary optics for each patient. Hundreds if not thousands of patients who cannot otherwise see, and/or to avoid intolerable photophobia and ocular suffering or corneal surgery, have benefited. With the growth of various lens designs and increase in clinicians who can provide such lenses, distribution and costs should be enhanced.
We must recognize, however, that the numbers of such lens fits will remain limited as we have so many other, easier to fit, and less costly devices to serve most of the contact lens-wearing population.
Advances in Presbyopia Management
As a clinician, I am aware that over the past decade, there has been another slowly but definitely incrementally improving area of subspecialization: that of presbyopic contact lens correction. The people to whom we clinicians, and our patients, owe thanks for this development are mostly unknown (at least not known to me) optical engineers and designers at large and small contact lens manufacturers who have developed relatively successful presbyopic lens designs for (primarily) simultaneous vision through a slow iterative process.
When I consider previous designs and how poor they were (optically speaking) several years ago, I am legitimately impressed. I suspect that as successful cases increase, so will interest in this area on the part of both patients and clinicians and that multifocal lenses have the potential to become very popular and widespread in application.
Advances in Flexible Contact Lenses
It is also absolutely clear that we have passed, almost without fanfare, another barrier with the proliferation of high-oxygen-permeable silicone hydrogel soft lenses over the past decade. It's been a relatively fast journey from a very few obviously stiff and rough-edged lenses that offered only one advantage (high Dk) to a large variety of soft, comfortable designs that also provide excellent optics (both spherical and toric) and tolerance, from multiple competing manufacturers.
One question, yet argued, is that of the critical oxygen needed for acceptable human use. After much consideration of the literature, I personally feel a good (and simple) number for us to bear in mind is 100. If the contact lens has an oxygen transmission value (Dk/t) or Dk approaching 100 Fatt units, or provides an underlying tear oxygen tension of about 100mmHg, or close to such a value, it will probably be physiologically tolerated by most eyes for daily wear (Weissman and Ye, 2006).
As shown by Schein et al (2005) and others, however and unfortunately, high Dk alone will still not solve the issue of physiologically tolerable extended wear. I believe that to achieve viable extended wear we will have to dramatically enhance our understanding of ocular immunology. This might be a very good development, not only for the (to my mind) relatively trivial goal of achieving extended wear as safe as daily wear, but also to enhance our abilities to manage and treat all varieties of ocular infection and non-infectious disease.
I must add that I am also very impressed with the introduction of both physiologically and optically effective custom soft silicone hydrogel designs for those few patients who cannot be helped by the mass-produced molded lenses.
Advances in Myopia Treatment
Another area of slow, incremental progress has been in the linked—but not precisely the same—endeavors of myopia prevention and treatment. Undoubtedly stimulated by both the developments in refractive surgeries and parents eager to offer their children options to avoid both the cosmetic/optical as well as ophthalmic disease consequences of myopia progression, research has slowly begun to understand both myopia development and appropriate preventive and therapeutic interventions.
Both “traditional” and newer paradigms of orthokeratology were directed at the use of GP lenses to reshape the anterior corneal surface. Orthokeratology was limited in effect, and may have suffered from cost effectiveness. Also, some potential hazard continues with extended wear of orthokeratology lenses(Lu et al, 2001).
Now with science being led by such visionaries as Dr. Earl Smith, we are learning that peripheral retinal myopic defocus may be the driving mechanism leading to progressive myopia; so peripheral hyperopic defocus (caused by ortho-k lens designs and those similar to concentric bifocals) could be effective in reducing the stimulus to myopic progression. As evidence gathers, confirmation of this paradigm should allow the development of treatment designs, both in spectacles and, more likely, in contact lens formats, that will be both better accepted and more cost effective.
Advances in Dry Eye
Whenever contact lenses are discussed, those who bemoan the lack of growth in wearers cite the dual issues of dry eyes/end-of-day lens discomfort and inadequate presbyopic correction. I already have discussed my personal impression of enhancement in presbyopic lens optics. Similarly, there have been some, but admittedly not as impressive, advances in diagnosing and then treating subjective and objective tear deficiencies. To my mind, the “breakthrough” here has yet to come but is anticipated, and certainly incremental progress is ongoing.
I believe that we will find that there are many types of dry eyes, not just one, and each will require a somewhat different treatment paradigm. How many of you have experienced, as I have, occasional patients who have very low tear breakup times and/or Schirmer results but still demand, and surprisingly well tolerate, contact lenses without subjective or objective complications?
Certainly we encounter terrible dry eye conditions, some primary, some secondary, that can lead to ocular surface compromise. Most of these patients should not wear cosmetic contact lenses, but even some will benefit not only optically but physiologically from therapeutic lens wear, often with GP sclerals. Milder dry eye states “merely” complicate any desired lens wear often without clinical signs, leading to symptoms and failure to tolerate contact lenses with subsequent “dropout.” Also, some patients only suffer dry eye clinical signs and symptoms when wearing contact lenses.
These latter two groups can be helped, perhaps, by treatments that we now know include lid hygiene, artificial tear supplementation, nutritional modification, perhaps local immunomodulation, and perhaps tear drainage duct punctal occlusion. As our understanding improves, I suspect, so will our diagnostic and management/treatment paradigms.
Advances in Inflammation Treatment
When I graduated optometry school in 1972, most clinicians thought that extending contact lens wear through one or more overnight (sleep) cycles could be physiologically dangerous, but we all saw the occasional patient who, over our objections, would tell us of such experiences without much effect. In my experience, I recall patients who suffered substantial corneal vascularization following noncompliant PMMA contact lens wear—or use of thick edged e.g. toric soft lenses (Figure 2)—but I recall no corneal infections from such contact lens use.
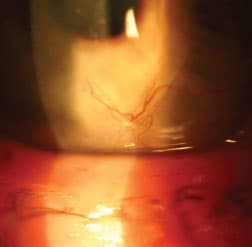
Figure 2. Corneal neovascularization associated with soft lens wear over a corneal transplant.
When soft lens extended wear became a popular modality a decade later, however, it did not take long before emergency rooms saw a dramatic increase in patients presenting with corneal infections primarily associated with extended wear. I know, because I was there (Weissman et al, 1984). This experience continues today (Lee et al, 2011) (Figure 3).

Figure 3. Pseudomonas sp. proven microbial keratitis associated with soft lens wear.
At first manufacturers thought that lens disposability would solve this problem by eliminating exposure to potentially contaminated and/or toxic solutions. Then, when this first paradigm failed, enhanced oxygen permeability (silicone hydrogels) became the proposed “Holy Grail” answer. Unfortunately, while both advances resulted in improved lens tolerance and much improved corneal physiology, neither has changed the rate at which microbial corneal infection occurs during extended wear (Schein et al, 2005).
We are making progress in understanding the pathophysiology of several types of corneal infection thanks to researchers such as Drs. Suzanne Fleiszig (2010), Charlotte Joslin (2010), and Mark Willcox (2011). However, for an obscure reason or reasons, it is clear that lens wear extended through one or more sleep cycles increases bacterial corneal infection risk, especially with the gram negative bacteria Pseudomonas sp. Fleiszig has proposed that the in-vivo corneal surface has many interacting anti-bacterial defenses only surmounted by multiple failures and microbes “educated” by exposure of some time length to our cells. Such advances in our understanding may soon change the way we manage patients to preclude such events as well as the way we treat patients suffering such disease.
Acanthamoeba sp. (not a bacteria, but a protozoa) keratitis infections (AK) are more associated with poor lens care, especially exposure of the lenses and/or cases to non-sterile waters, than with extended wear. Although it is clear that AK is a very rare event, it is catastrophic for patients: horribly painful and often blinding. Well-known failures of two multipurpose lens care solutions since withdrawn from the contact lens marketplace have added to our understanding of how to protect patients from such risks.
In addition to our enhanced understanding of both avoidance and treatment strategies, research suggests that pre-immunization may be a most successful management strategy for AK in particular (Alizedeh, 1995).
Gell and Coombs (1963) organized our understanding of non-infection driven inflammation into four types, the first of which is classic allergy, a mast cell-IgE mediated response. Other distinct and different forms of hypersensitivity commonly encountered during contact lens practice include contact derma-titis. Toxicity is distinguished by being a non-immunological mediated broad spectrum reaction to a universally noxious substance. Allansmith et al (1977) recognized the initial Gell Combs type 1 ocular complication of contact lens wear (giant papillary conjunctivitis), but as the era of hypoxia fades, the era of immune response surfaces.
The understanding of this collection of responses that lead to similar types of suffering in the eyes and adnexa (conjunctival injection, discharge, itching, burning, etc.) is complicated by the interwoven and still poorly understood role of tear insufficiency (dry eye) and by the danger of possible clinical confusion with direct microbial infection. We are slowly learning more and un-teasing more parts of this puzzle.
The clinician's role is to first distinguish non-infectious immune response from infection. Ocular infection must be treated aggressively and appropriately to reduce the risk of vision loss through corneal scarring/distortion and further damage to other ocular structures. If ocular infection has been eliminated from the differential diagnosis, then reducing the signs and symptoms of often inappropriate non-infectious driven immunological response becomes the clinician's objective (Figure 4).
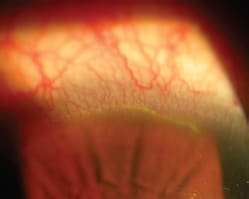
Figure 4: Non-infectious superior epithelial arcuate lesion (SEAL) seen in a myopic silicone hydrogel lens wearer's eye.
Fortunately, we are gaining many enhanced pharmacological tools to assist us in managing non-infectious inflammation, including mast cell stabilizers, antihistamines, and immunomodulators. I suspect that the pharmologic industry will provide us, and our patients, with ever more finely directed drugs as we progress into the 21st century. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #198.