


MYOPIA CONTROL
Current and Future Developments in Myopia Control
Researchers continue to seek effective methods to slow the progression of myopia.

| Dr. Walline is an associate professor at The Ohio State University College of Optometry. He teaches pediatrics and specialty contact lenses, and he conducts pediatric contact lens research. He has received research grants from CooperVision and Alcon Laboratories Inc. and lecture and authorship honoraria from Johnson & Johnson Vision Care. |
By Jeffrey J. Walline, OD, PhD, FAAO
Before beginning any discussion of myopia control, we must first establish what we consider to be clinically meaningful control. In the United States, the average rate of myopia progression in children is about 0.50D a year (Fulk et al, 2000; Gwiazda et al, 2003; Walline et al, 2004; Walline et al, 2008). For example, if a child is diagnosed with 1.00D of myopia at age 8 and his refractive error progresses linearly at the average rate and then stops at age 16, he will become a –5.00D myope. Reducing myopia progression in this child by 25 percent, 50 percent, 75 percent, or 100 percent would result in the final refractive errors shown in Table 1. Anecdotally, most eyecare practitioners who discuss this topic at meetings around the world believe that myopia progression must be slowed by at least 50 percent to be clinically meaningful for patients.
| TABLE 1 | |
|---|---|
| What Is Meaningful Myopia Control? | |
| If myopia progression is slowed by | Final myopia would be |
| 0% | –5.00D |
| 25% | –4.00D |
| 50% | –3.00D |
| 75% | –2.00D |
| 100% | –1.00D |
| In this theoretical example, a child was diagnosed with 1.00D of myopia, which progressed exactly –0.50D per year for eight years. The final refractive error is shown for each percentage of slowed myopia progression. | |
Two Decades of Trials
Researchers have experimented with numerous methods to slow myopia progression (Table 2). If we agree that progression must be slowed by at least 50 percent to be clinically meaningful, then most of these methods—undercorrection of myopia, alignment-fit GP contact lenses, bifocal or multifocal spectacles, spectacles that create myopic blur in the periphery, and pirenzepine—have been ineffective.
| TABLE 2 | |||
|---|---|---|---|
| Myopia Control Studies, Categorized by Agent | |||
| Method | Author (year) | % reduction* | Overall Average** |
| Undercorrection | Aller (2006) | –16 | –19 |
| Chung (2002) | –22 | ||
| Alignment gas permeable lenses | Katz (2003) | –5 | –7 |
| Walline (2004) | –8 | ||
| Bifocal or multifocal spectacles | Edwards (2002) | 3.1 | 18 |
| Fulk (2000) | 20 | ||
| Gwiazda (2003) | 16 | ||
| COMET2 (2011) | 24 | ||
| Cheng (2010) | 32 | ||
| Yang (2009) | 14 | ||
| Hasebe (2005) | 18 | ||
| Peripheral myopia spectacles | Sankaridurg (2010) | 30 | 30 |
| Pirenzepine | Siatkowski (2008) | 30 | 35 |
| Tan (2005) | 39 | ||
| Corneal reshaping | Cho (2005) | 44 | 46 |
| Kakita (2011) | 36 | ||
| Walline (2009) | 58 | ||
| Soft bifocal lenses | Sankaridurg (2011) | 34 | 51 |
| Aller (2006) | 79 | ||
| Walline (2011) | 40 | ||
| Anstice (2011) | 50 | ||
| Atropine | Chua (2006) | 77 | 81 |
| Shih (1999) | 96 | ||
| Yen (1989) | 76 | ||
| Fang (2010) | 76 | ||
| *Negative numbers indicate an increase in myopia progression. | |||
| **Overall average is a simple mathematical average of each of the studies, not weighted by sample size or any other considerations. | |||
By far, the most effective agent for slowing myopia progression is atropine, but eyecare practitioners rarely prescribe it, primarily because they believe that its side effects of mydriasis and cycloplegia are uncomfortable for children. Interestingly, dropout rates from myopia control studies using atropine (Shih et al, 1999; Shih et al, 2001; Chua et al, 2006) are significantly lower compared to dropout rates from most studies using alignment-fit, daily wear GP contact lenses (Baldwin et al, 1969; Perrigin et al, 1990; Khoo et al, 1999; Katz et al, 2003). This may indicate that atropine is not as uncomfortable for children as many practitioners believe, especially if the children wear multifocal spectacles with photochromic lenses. There is evidence, however, that the accrual of a treatment effect from atropine does not continue after the first year (Figure 1), and short-term use of atropine may not lead to a permanent treatment effect. In addition, we do not know the effect of atropine after long-term use, specifically through the age at which we expect myopia progression to cease naturally.
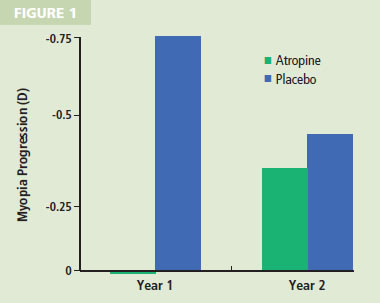
Figure 1. Myopia progression by year for eyes receiving atropine compared with eyes receiving placebo. Note the slight regression of myopia (0.03D regression) for the atropine eyes and the significant myopia progression for the placebo eyes in year 1. Progression is similar in each group during year 2 of the study.
Of the other myopia control treatments studied thus far, only two yield the requisite 50 percent treatment effect: corneal reshaping contact lenses and soft bifocal contact lenses. Any discussion of these therapies must be tempered by the fact that no long-term, randomized clinical trials have been reported in the peer-reviewed literature to firmly establish their role in myopia control.
Contact Lens Therapy
Evidence from myopia studies in primates indicates that hyperopic blur presented to the retina increases eye growth (Smith et al, 2009). By extension, it is hypothesized that myopic blur presented to the peripheral retina will decrease eye growth. Based on that hypothesis, some researchers theorize that corneal reshaping contact lenses and soft bifocal contact lenses that have a center-distance design may slow myopic eye growth. Studies of these two lens types have produced encouraging results.
Evidence of a continued accrual of treatment effect exists for corneal reshaping contact lenses (Cho et al, 2005; Kakita et al, 2011), but studies of soft bifocal contact lenses have not been of sufficient duration to replicate this finding. Further-more, myopia control studies of atropine therapy (Chua et al, 2006) and of multifocal spectacles have failed to show an accumulation of treatment effect (Gwiazda et al, 2003). It is unknown why some studies may show an accrual of treatment effect whereas others do not.
Studies of corneal reshaping contact lenses have shown that subjects who have higher myopia experience greater slowing of myopia progression (the higher the myopia, the greater the effect), whereas control subjects with higher myopia who wear single vision spectacles do not experience slower myopia progression (Kakita and Cho, 2005). This may indicate that greater myopic blur presented to the peripheral retina may provide better myopia control. If that is the case, then soft bifocal contact lenses that have greater add powers would be expected to slow myopia progression more than would soft bifocal lenses that have lower add powers.
Children are capable of wearing either corneal reshaping lenses or soft bifocal lenses (Walline, 2009; Cho, 2005; Sankaridurg, 2011; Anstice and Phillips, 2011; and others—complete list available at www.clspectrum.com/references.asp), and evidence suggests that these contact lenses may incorporate the added benefit of myopia control, so why not fit children with these lenses?
Prescribing for Children
The decision of whether to fit a child with corneal reshaping contact lenses or soft bifocal contact lenses should be made after a discussion between the eyecare practitioner, the parents, and the child. Several factors help determine the best option, such as the practitioner's comfort with fitting each lens type, the child's perceived ability to handle contact lenses, and the parents' comfort with either type of lens. Some specific considerations include:
• Child's Activities Children who swim regularly, for example, would benefit from corneal reshaping contact lenses, which would not be worn in the swimming pool and, therefore, are less likely to be contaminated by microbes that may be found in pool water.
• Preference for Part-Time Wear A child who wants to wear contact lenses only part-time during recreational activities is a better candidate for soft contact lenses, although the myopia control aspect of part-time wear is unknown.
• Parents' Preferences Parents who are uncomfortable with their children wearing contact lenses outside of the home should consider corneal reshaping lenses, while parents who currently wear soft lenses may be more comfortable having their children wear something similar.
Eyecare practitioners report that they are fitting children with contact lenses at earlier ages in large part because of improved oxygen permeability and the availability of daily disposable lenses (Sindt and Riley, 2011). Although no center-distance daily disposable bifocal contact lenses are available, this design is available in silicone hydrogel materials.
Safety Considerations
Bullimore (2009) reported that rates of microbial keratitis were no higher in patients wearing corneal reshaping lenses than they were in patients wearing soft lenses overnight (Stapleton et al, 2008). This suggests that corneal reshaping lens wear poses no greater risk of microbial keratitis due to thinning of the corneal epithelium than does the risk imposed by overnight lens wear. Furthermore, many cases of microbial keratitis associated with corneal reshaping reported in the literature occurred in East Asia in 2001 before strict regulations for fitting corneal reshaping lenses were implemented, and the cases were associated with Acanthamoeba keratitis (Watt and Swarbrick, 2007). These factors indicate that poor management and poor lens care contributed to many cases of eye infections associated with corneal reshaping lenses, and that diligent care and monitoring will minimize the risk of infection.
Research Continues
Even if scientists confirm that myopic blur presented to the peripheral retina slows myopia progression, they still must determine what optimizes the signal to slow eye growth. Does the eye regulate its growth to provide the clearest visual input? If so, should we try to minimize peripheral higher-order aberrations, or is it sufficient to minimize peripheral astigmatism? Does the retina respond primarily to the maximum myopic blur presented to the periphery, or is it more important to present myopic blur to the greatest area of the retina? As they seek answers to these questions, scientists are exploring numerous avenues to slow myopia progression including some that do not involve optical means such as genetic manipulation, therapeutic eye drops, and filtering of specific wavelengths with colored lenses.
| Myopia Progression in Adults |
|---|
| Therapies to control myopia progression are primarily tested in children because most myopia manifests before puberty, and progression is much faster in young patients. Myopia onset or progression is also possible in young adults, however, and studies of potential treatments for these patients are also important. It may seem logical to assume that the optical properties of contact lenses that are thought to slow myopia progression in children would extrapolate to young adults, but this may not be the case. There may be a period of plasticity that expires over time, thus reducing or eliminating the myopia control benefits of corneal reshaping or soft bifocal contact lenses for adults. We still have much to learn about adult-onset myopia and progression before we can begin to consider treatments to control it. |
The goal of each therapy is to slow the progression of myopia by at least 50 percent. Some may ask: What is the difference for a patient whether his prescription is –3.00D or –5.00D? Either way, he will still require vision correction to see optimally. We already know of numerous potential benefits. Perhaps by slowing the growth of the eye, we can lower the risk of retinal detachment, cataract, glaucoma, or chorioretinal degeneration (Saw et al, 2005). More likely, we will improve the patient's quality of life (Rose et al, 2000). Patients who have less myopia are also better candidates for refractive surgery because they experience more repeatable, accurate results (Lin and Tsai, 2005).
As we continue to learn about the mechanisms that regulate eye growth, we may eventually be able to apply our knowledge to preventing the onset of myopia.
Today's Best Options
Given what we know now, the best options for myopia control may be soft bifocal and corneal reshaping contact lenses. Children as young as 8 years old should routinely be offered these two types of correction. We know that they are capable of safely wearing and caring for contact lenses (Soni et al, 1995; Walline et al, 2004; Cho et al, 2005; Walline et al, 2007; and others), and contact lens wear may improve their perceptions of their appearance as well as their athleticism and peer interactions (Walline et al, 2009). Contact lens wear may also provide the added benefit of slowing the progression of myopia.
Many parents assume that their children will not be able to wear contact lenses until their teen years, so it is important for eyecare practitioners to proactively discuss contact lenses with young children and their parents. Although we should not unequivocally state that corneal reshaping lenses or soft bifocal contact lenses that have a center-distance design will slow myopia progression, we can discuss the benefits of contact lens wear such as improved quality of life in the areas of participating in recreational activities and appearance while wearing vision correction (Rah et al, 2010). At the same time, we can tell parents that these contact lenses may also have the beneficial side effect of possibly slowing the progression of nearsightedness for their children. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #203.