


October 2012 Online Photo Diagnosis
By William Townsend, OD, FAAO
This 22-year-old college student presented complaining of reduced vision in her right eye. She had minimal discomfort, reporting occasional episodes of dryness more apparent in her affected eye. She denied any trauma, but admitted to occasionally wearing her daily wear lenses overnight. She denied using any OTC or prescription drops since she began to have poor vision.
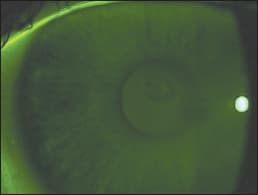
Presenting corrected visual acuities were: OD 20/25 and OS 20/20. Over-refraction did not further improve her vision. After removing her lenses, biomicroscopy revealed a perfectly circular area of negative staining positioned directly over the visual axis. No infiltrates or breaks in the epithelium were apparent. The anterior chambers were devoid of cells or flare, and there was no conjunctival injection.
Our initial impression was a focal area of epithelial edema, most likely due to lens over-wear. We instructed the patient to totally discontinue contact lens wear or, because she was a collegiate athlete, to wear the lenses only during games. We put her on a regimen of 5% hypertonic drops during the day and 5% hypertonic ointment at bedtime.
The patient returned in one week and reported that her vision was worse, but that she still had no pain or discomfort. She reported wearing her lenses on a very limited basis, for games and practice. Corrected acuities were: OD 20/30 OS 20/20. Examination revealed virtually no change in elevation of the lesion, which we confirmed by corneal topography. A new finding was the presence of sub epithelial infiltrates directly beneath and limited to the area of the lesion, which was still perfectly round in shape. Our new diagnosis was corneal infiltrate underlying a focal discrete area of epithelial edema. We instructed the patient to continue the hypertonic therapy but added Lotemax (Bausch + Lomb) ophthalmic suspension every four hours in the affected eye.
One week later, the lesion was so much improved that it was difficult to ascertain where it had been. We instructed the patient to taper the steroids and to continue the hypertonic therapy for two weeks.
One of the lessons I gleaned from this case is that in clinical practice we may encounter conditions that cannot be “named.” We may never know the exact cause of the lesion, but we can look for several important attributes and treat the condition accordingly. I first asked myself if this patient's condition resulted from an infection. Infectious processes are usually easy to treat, once the precise cause (bacterial, viral, etc) has been established, but in this case infection was highly unlikely. The second question I asked was, “Is this an inflammatory or degenerative process?” Initially the answer to both questions was no, but after the appearance of the infiltrates, I recognized that there was an inflammatory component and treated it based on that finding. Fortunately, the condition responded as I had hoped, and the patient regained good vision and normal function.
In managing ocular disease, we are taught to “pin down” a diagnosis, i.e. XXX syndrome, or SSS dystrophy. But in real life, we may encounter conditions that elude “diagnosis” — and yet we are able to successfully treat them based on observation of signs and symptoms as well as our understanding of the principles of disease management.