


SCLERAL COMPLICATIONS
Solving Scleral Lens Complications
This illustrated guide can help correct and avert adverse events with large-diameter lenses.

| Dr. Jedlicka is owner and director of the Cornea and Contact Lens Institute of Minnesota, Edina, Minn., and secretary of the Scleral Lens Education Society. E-mail him at jgjod@yahoo.com. |
By Jason Jedlicka, OD, FAAO
Scleral contact lenses can be a wonderful, life-changing option for patients who have irregular corneas or ocular surface disease. However, like any other lens, complications can arise with the lenses themselves or with patients' ocular health. All scleral lens fitters from time to time will encounter complications as a normal part of practice.
Most complications occur through problems with lens design or lens care and application. Lens fit concerns are more common for inexperienced fitters. As your scleral fitting experience increases, your fitting complications will lessen.
Care and Application Complications
Complications with lens care and application are most common among beginning wearers. At each follow-up visit, it is important to address proper care and handling as well as proper care solution use to ensure that patients have a clear understanding of lens care. Sometimes a new scleral lens wearer is consumed with application and removal and is unable to concentrate on proper lens care. It's a good idea to readdress care when the patient is better able to focus on the instructions. Technicians should reinforce lens care instructions as well.
Make it a standard part of every follow-up visit to ask patients what they use for cleaning, storing, rinsing, and filling their scleral lenses. This is more important with scleral lenses than with standard GPs because what is beneath a scleral lens at application stays there for hours while what's beneath a standard GP lens is gone within five minutes.
Lens Design Complications
Lens design complications frequently are not detected during the initial fit because they tend to occur over time. Obvious design problems are evident during the fitting process, and the fit can be changed to avoid them. But more subtle fitting complications that develop with wearing time will need to be evaluated at follow-up visits. Letting patients know at the dispensing appointment what they should watch for or what symptoms they may experience can prepare them to contact your office should a complication develop. Some examples of symptoms might include increasing redness with lens wear, lens tightening, light sensitivity, or irritation after lens removal.
To detect these problems, it's advisable to schedule follow-up visits with scleral lens patients later in the day or to have patients wear the lenses for at least three to four hours prior to the visit. This allows time for any redness to appear. At follow-up visits, assess the eye with the lens in situ prior to application of fluorescein or prior to removing the lens and reapplying with fluorescein. Make full notes of the fit as-is, checking for sinking and settling prior to manipulating the lens. Next, add fluorescein to see how readily it exchanges under the lens. If necessary, remove the lens and reapply with fluorescein to assess the fit yet again.
Many novice fitters want to immediately view the fluorescein pattern, as is the practice with standard GP lenses and requires removing the lens and reapplying with fluorescein. Don't be in a rush to add fluorescein. Evaluate the fit in all ways necessary prior to removing the lens and instilling fluorescein. Once the lens is removed, all opportunity for checking how the lens settles is lost.
Make lens design changes based upon the complication observed, such as flattening the peripheral curve or landing zone in a lens that exhibits edge compression or increasing the vault in a lens that bears on the cornea.
Visual Complications
Visual complications typically arise from residual astigmatism or from lens surface/tear chamber opacities such as debris or lens non-wetting. Address visual problems arising from surface deposits or non-wetting through care and handling discussions with affected patients.
If vision is reduced through residual astigmatism, it's necessary to determine whether the reduced vision is related to flexure or to true residual astigmatism. As a good initial step in trying to determine whether flexure is occurring, use a stiffer trial lens or reorder a lens with a significantly increased center thickness. If there is still residual astigmatism at this point, it can be corrected with a front-toric lens or with spectacles worn over the contact lenses.
Resolving Specific Scleral Complications
See Table 1 for a quick reference guide on the causes and remedies of scleral lens complications. Figures 1 through 7 illustrate many of the complications that arise with scleral lens fitting.
| TABLE 1 | ||
|---|---|---|
| Complications Quick Reference Guide | ||
| Problem | Causes | Remedy |
| Symptoms | ||
| Discomfort | Loose lens fit (initial discomfort) | Tighten lens edges / increase sag |
| Tight lens fit (later onset discomfort) | Loosen lens edges | |
| Inappropriate lens solutions | Verify proper lens care and application procedures | |
| Blurry vision | Lens flexure | Increase lens thickness / Switch to toric peripheral curves |
| Surface debris | See “lens surface debris” | |
| Tear layer debris | See “tear layer debris” | |
| Air bubbles under lens | See “air bubbles” | |
| Lens Complications | ||
| Air bubbles | Improper application technique | Reinstruct on proper application technique |
| Poor lens fit / Incomplete seal | Evaluate fit for possible need for increased sag or toric / quadrant-specific periphery | |
| Fenestration | Remove fenestration | |
| Seal-off | Lens is too steep in the periphery | Flatten back surface peripheral curves of the lens central to the area of blanching / compression |
| Lens is too thin / flexes | Increase lens thickness | |
| Conjunctival blanching | Steep periphery if at lens edge | Flatten peripheral curves to more evenly distribute lens bearing |
| Flat periphery if inside lens edge | Steepen peripheral curves to more evenly distribute lens bearing | |
| Asymmetric scleral if sectoral | Consider toric or quadrant-specific peripheral curves | |
| Lens adherence | Lens flexure | Increase lens thickness |
| Insufficient corneal / limbal clearance | Increase vault where needed to ensure sufficient vault in | |
| Significant lens settling | Increase vault / Remove fenestration if utilized | |
| Lens drop | Toric sclera | Utilize toric peripheral curves |
| Excessive vault | Decrease vault if possible | |
| Excessive lens mass | Decrease lens diameter / decrease center thickness | |
| Lens surface debris / non-wetting | Poor cleaning / care habits | Instruct on proper care / Polish lenses / Plasma treatment |
| Meibomian gland dysfunction (MGD) | Lid hygiene / Topical or oral medication for MGD | |
| Manufacturing defect / residue | Try lab cleaning. If ineffective, have lens remade or plasma treated | |
| Tear layer debris | Poor tear quality | Remove lens / Rinse / Reapply as needed |
| Excessive corneal vault | Lower vault if excessive and if possible | |
| Excessive lens edge / conjunctival interaction | Modify lens edge to minimize bulbar and palpebral conjunctival “rubbing” | |
| Ocular Complications | ||
| Hypoxia / Edema | Insufficient oxygen transmission | Increase lens material Dk if possible or decrease center thickness if possible |
| Insufficient tear exchange | Verify proper fit and tear exchange | |
| Redness | Hypoxia | See “hypoxia” |
| Toxicity / Debris | Verify proper solutions. If significant debris, consider steepening the peripheral curves to avoid lens / lid interaction | |
| Corneal mechanical breakdown | Increase corneal clearance in area of lens corneal contact | |
| Corneal staining | Lens contact with cornea (localized to area of contact) | Increase lens vault in areas of contact |
| Toxic tear layer / Debris (generalized) | Increase tear exchange if lens appears too tight. If edges appear loose, steepen periphery to reduce debris | |
| Improper application (local but not in area of contact) | Reinstruct on proper application techniques | |
| Hypoxia | See “hypoxia” | |
| Conjunctival staining | Dryness | Larger diameter lens / Lubricant drops / Toric peripheral curves |
| Conjunctival loose tissue | Loose conjunctiva | Can surgically excise, but unnecessary unless corneal neovascularization develops |
| Solution hypersensitivity | Use of inappropriate / noncompatible solutions | Verify proper care products including non-preserved solutions in lens bowl |
Figure 1 shows a toric scleral lens. Residual astigmatism that reduces visual acuity can be resolved by increasing center thickness, therefore reducing flexure, or it can be corrected by fitting a front-surface toric. These are fitted like any other scleral lens. The resultant sphero-cylindrical over-refraction can be ground onto the front surface of the lens and stabilized with a thin-zone or prismballast design. Front-toric lenses are typically marked to check for rotation. Compensate for rotation as with any other toric lens.

Figure 1. Toric scleral lens.
Surface deposits often occur more readily on the harder-to-clean back surface of a scleral lens. Surface deposits can cause decreased comfort and decreased acuity. Resolving this comes down to reviewing proper care and handling, using a GP lens cleaning product if the patient isn't already doing so, adding an extra-strength cleaner such as Progent (Menicon), or using a cotton tip applicator to better clean the inside back surface.
Many patients who wear scleral lenses have significant ocular surface disease and therefore are at greater risk for surface wetting problems (Figure 2). In addition, traditional GP materials that enhance lens wettability are generally avoided with scleral lenses, which does not help matters. Scleral lenses that have a significant degree of vault will extend beyond the typical front ocular surface. By pushing the lens out further, dryness increases due to a larger surface area exposed to the air. Resolve this problem by making sure that patients clean lenses well, by treating any lid disease, or by reducing the vault if the lens is vaulting more than necessary. Consider having the lens plasma treated if you haven't already done so.

Figure 2. Scleral lens non-wetting.
Bubbles (Figure 3) can occur due to improper application or through an improper lens fit. If the lens fits properly, revisit application techniques with the patient. Lenses that develop bubbles after application will likely have at least one quadrant in which the peripheral curves are too flat. Consider toric peripheral curves or a quadrant-specific design.
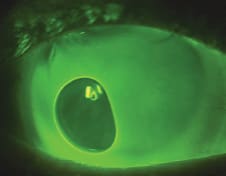
Figure 3. Bubble.
Flexure (Figure 4) can complicate scleral lens wear in two ways: through compromised vision due to induced astigmatism or through discomfort due to a progressively tightening lens. A lens that flexes will tighten more noticeably compared to a lens that resists flexure. When visual acuity with a scleral lens is less than expected, a sphero-cylindrical over-refraction can determine whether astigmatism is present. Significantly increasing the center thickness can reduce or eliminate flexure, leading to sharper visual acuity and a lens that resists tightening with wear.

Figure 4. Flexure.
Corneal staining can result from edema, solution toxicity, or a toxic tear layer from metabolic waste behind the lens. Resolve it by discussing use of proper lens care products with patients and by using materials with maximum oxygen transmission (Dk/t) values.
Another type of corneal staining occurs with lens-cornea touch from inadequate vault. Remedy this by refitting the scleral lens with increased vault.
Conjunctival hooding or folding (Figures 5 and 6) typically occurs in an eye in which the conjunctival tissue is loose or baggy. It is of no consequence unless corneal neovascularization occurs in the area where the folds are located. If so, lower the vault in that area of the lens fit.

Figures 5 and 6. Conjunctival hooding and folding.
Chamber debris can appear when the superior and inferior edges of the lens are too flat. It can affect vision and long-term comfort and may require removing the lens occasionally during the day to rinse and reapply. Steepening the peripheral curves or lowering the vault can sometimes help.
Blanching at the lens edge (Figure 7) is due to a tight peripheral curve or tight landing zone. Blanching can occur at 360 degrees if the curve is too steep, or it can be sectoral if the sclera is asymmetrical. It will often lead to redness after the lens is removed. Blanching requires flattening the edge curve or, for sectoral blanching, can be resolved with toric peripheral curves.

Figure 7. Blanching.
An Additional Scleral Lens Resource
A good resource for support and information about fitting scleral contact lenses is the Scleral Lens Education Society (www.sclerallens.org), a nonprofit organization committed to teaching contact lens practitioners the science and art of fitting all designs of scleral contact lenses for the purpose of managing corneal irregularity and ocular surface disease. CLS