


WAVEFRONT ERROR CORRECTION
Incorporating Wavefront Error Correction in Contact Lenses
State-of-the-art refractive surgery uses wavefront correction. Why not contact lenses?

| Dr. Marsack completed a PhD in physiological optics and vision science at the University of Houston, College of Optometry. His research interests include optical aberration of the eye, custom and pseudo-custom correction of optical aberration, visual performance, metrics predictive of visual performance, and ocular drug delivery. |
By Jason Marsack, PhD
In the contact lens world, wavefront error and wavefront-guided correction tend to be regarded as separate from refractive error and refractive correction. In a clinical context, the term wavefront is often associated with costly instruments and complex mathematical reporting schema, which adds to the misperception that wavefront error and refractive error are separate quantities.
In fact, the two are intimately related. We find evidence of this relationship in state-of-the-art refractive surgery that incorporates wavefront error measurements to target both lower-order aberration (spherocylindrical refractive errors) and higherorder aberration (HOA) (spherical aberration, coma, trefoil, etc.) in the correction.
If wavefront error correction is integral to successful refractive surgery, a logical question from a contact lens perspective is: Could wavefront technology be routinely employed in contact lens practice to benefit patients and practitioners? In this article, I explore the potential for wavefront error correction in contact lenses.
Wavefront Error Defined
In clinical practice, the term refractive error usually means spherocylindrical error and is most frequently quantified through refraction with a phoropter or trial lenses. However, spherocylindrical error represents only a subset of the refractive errors of the eye. Researchers have established that nonspherocylindrical errors also exist in normal eyes (Howland et al, 1977; Porter et al, 2001). Fortunately, nonspherocylindrical errors usually have a minimal impact on the visual performance of normal eyes, and patients usually achieve excellent vision with spherocylindrical corrections based on subjective refraction.
Subjective refraction does not represent all of the visually important refractive errors of highly aberrated eyes such as those that have keratoconus, pellucid marginal degeneration, ocular trauma, and suboptimal refractive surgery outcomes. In these cases, wavefront error measurements more accurately describe the optical errors that may limit visual performance. In other words, these highly aberrated eyes may gain significant retinal image quality when HOAs are adequately corrected.
Measuring Wavefront Error
Spherocylindrical refractive error is reported in diopters (sphere and cylinder) and degrees (axis), but wavefront error requires a more extensive reporting method. Common conventions have been established to report wavefront error, in particular the use of the Zernike polynomial to report individual aberrations, standardized as ANSI Z80.28-2004. The Zernike polynomial is an effective method for reporting individual aberrations such as sphere, astigmatism, coma, etc., but clinically speaking, assessing the overall aberration structure can be difficult when it is communicated as a large list of numeric data. Wavefront error mapping is one of several methods used to summarize and interpret wavefront error data. The three-dimensional, color-coded maps report the difference between a reference wavefront and the measured wavefront for an eye, quantifying wavefront error over the pupil of the eye.
Figure 1 shows a series of wavefront error maps for an eye that has keratoconus. Figure 1a shows the portion of the wavefront error associated with defocus. This error is rotationally symmetrical and would be well corrected with a spherical soft contact lens. Figure 1b shows the addition of the astigmatic portion of the wavefront error. Although more complex, displaying mirror symmetry, this error would be well corrected with a spherocylindrical contact lens. Figure 1c shows the full wavefront error measured in this keratoconic eye, notably the prominent rotational asymmetry. Even after correcting the spherocylindrical errors, significant HOA (in this eye, coma) would remain and would continue to degrade retinal image quality.
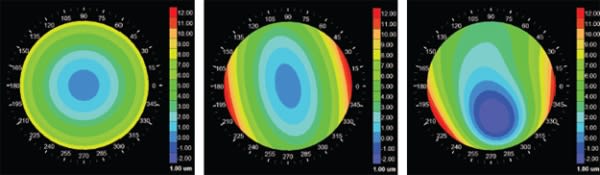
Figure 1. This series of maps of a keratoconic eye shows the myopic component of the wavefront error (1a), the inclusion of cylinder (1b), and the full wavefront error including higher-order aberration (1c). Wavefront error maps are defined over the pupil, giving them their round shape. Positive/negative wavefront error refers to a portion of the measured wavefront that is leading/lagging relative to the reference wavefront, and is represented in the color-coded scheme by red/blue colors.
Pantanelli et al (2007) reported that HOA levels in the keratoconic eye are roughly 5.5 times higher than those in the normal eye. Spectacles leave visually significant levels of refractive error (notably HOA) in the optical system, and this is one reason why spectacle correction does not consistently provide keratoconus patients with excellent visual acuity. Corneal scarring also plays a role in reducing visual performance in keratoconus, but the effects of scarring cannot be mitigated via the wavefront compensation described here.
HOA Compensation in a Contact Lens
All contact lenses correct some wavefront error. Spherical soft lenses, for example, are designed to correct defocus, but they do not target cylindrical errors and HOAs. Spherocylindrical soft lenses correct sphere and cylinder, but not HOAs. Because spherocylindrical refractive error comprises most of the visually significant wavefront errors in normal eyes, soft contact lenses usually provide excellent visual performance. As with spectacles, however, the benefit of spherocylindrical soft contact lenses in correcting highly aberrated eyes is limited. This is because the altered morphological characteristics of the refracting surfaces of these eyes lead to increased levels of HOA and decreased retinal image quality. For example, the downward displacement of the corneal apex in keratoconus leads to induced negative vertical coma (Pantanelli et al, 2007).
For patients who have keratoconus, GP contact lenses are the most common form of optical correction (Zadnik et al, 1998). The rigid nature of GP lenses provides the eye with a new first-refracting surface, and the tear lens film between the lens and the diseased cornea masks a portion of the HOA present in the eye. Although these lenses reduce the HOAs present in a keratoconic eye, they do not fully eliminate them, nor do they allow for quantitative, targeted correction of these aberrations. In other words, practitioners do not prescribe GP lenses to compensate for specified levels of HOA measured in the eye. Rather, they rely on the indexmatching properties of the tear film and the new rigid first surface of the optical system to reduce HOA. The result is incomplete correction of HOA and residual uncorrected errors that reduce visual performance (Marsack et al, 2007; Kosaki et al, 2007; Negishi et al, 2007). Although I have been discussing GP lenses for keratoconic eyes, a similar explanation applies to most corrections available for highly aberrated eyes: residual HOA remains in the system, with varying impact on visual performance.
Investigators for the Collaborative Longitudinal Evaluation of Keratoconus study reported that 77.9 percent of keratoconus subjects had 20/40 or better entrance visual acuity in both eyes, which suggests that current forms of correction do a reasonable job of providing good visual acuity in this population (Zadnik et al, 1998). Is it possible to deliver better image quality for such highly aberrated eyes?
One method currently under investigation is the targeted correction of higher-order optical aberration using wavefront error measurements. The concept has been under investigation for a number of years, with several groups demonstrating the principle that targeting HOA can lead to improved optical quality and visual performance.
Patient-Specific HOA Correction
Researchers have demonstrated the benefits associated with targeting HOA for correction with a custom contact lens on highly aberrated eyes using various methods. For example, Sabesan et al (2007) demonstrated that a wavefront-guided soft contact lens reduced HOA in keratoconus by a factor of 3. This type of lens uses the measured aberration of an individual eye and compensates for that error in a customized lens (Figure 2). Each lens is intended for wear on only one eye of one patient and is, therefore, a truly custom form of correction. In their study, Sabesan et al found that custom correction of HOA in keratoconus resulted in visual acuity improvement of 2.1 lines as compared with spherocylindrical correction alone.
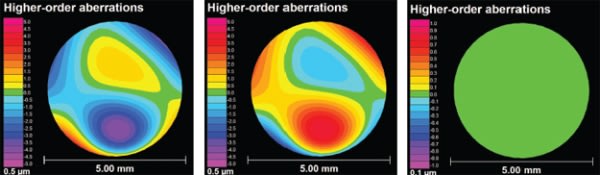
Figure 2. This series of images is a simulation of the intent of targeted HOA compensation in a contact lens. Figure 2a shows the higher-order aberration of a keratoconic eye. Figure 2b shows the optical compensation that would completely mitigate the measured wavefront error. This would result in the wavefront error shown in Figure 2c, in which the entire patch is green, representing no residual HOA present in the eye. Achieving this level of correction on a real eye would be complicated by a host of factors, such as wavefront measurement error, lens manufacturing error, lens movement, and physiological fluctuations in the wavefront error over time.
When considering the clinical utility of wavefront-guided custom contact lenses to correct HOA, it is important to consider how the lenses would perform relative to the gold standard form of correction: GP lenses. Marsack et al (2008) demonstrated correction of keratoconus with a wavefront-guided soft contact lens and compared the resultant visual acuity to that achieved with habitual GP lens corrections. In this experiment, all three subjects achieved photopic high-contrast logMAR visual acuity equal to or better than values recorded with their habitual GP contact lenses.
Implementing custom correction with a soft contact lens is complicated by the movement of the lens on the eye. To reduce the impact of lens movement and to provide a more stable platform for customization, researchers have begun to investigate the use of wavefront-guided optics on a scleral contact lens. Yoon et al (2011), working with Perry Rosenthal, MD, and The Boston Foundation for Sight, demonstrated custom scleral lens correction on 11 keratoconus patients. The researchers found that these lenses reduced HOAs and improved visual performance. The Visual Optics Institute at The University of Houston, College of Optometry is also investigating custom scleral lenses with corrections optimized for an individual eye.
The series of images in Figure 2 simulates how HOA can be targeted in a contact lens, the compensating correction and theoretical residual HOA when the correction is applied to the eye. Although these lenses have been studied, access to them in the clinical environment remains limited. However, there are ongoing efforts to move the technology to the clinic.
Adding to the Arsenal
What is the clinical potential of these patient-specific corrections designed from measured wavefront error? From the patients' point of view, these lenses would provide more complete optical correction, better retinal image quality, and a potential for improved visual performance. From the practitioners' point of view, these corrections provide another weapon in the clinical arsenal with which to treat the needs of their optically challenging patients.
The factors that lead to a successful contact lens fitting extend well beyond the image formed on the retina. Cost, wearing time, comfort, replacement schedule, and complexity of care regimen also must be considered. Because of these variables, I am convinced that all modes of contact lens correction will continue to have a place in practice. Each has inherent advantages that can make it better suited to individual patients. A good example of this is the renewed interest in fitting scleral contact lenses on highly aberrated eyes and eyes that have dry eye disease. Almost 125 years have passed since the first scleral lens demonstrations, and the field continues to find new utility for modern scleral lenses made of highly oxygen permeable materials. As wavefront technology begins to find application in contact lenses, it would seem logical that they will complement, not replace, existing contact lenses.
Summary
Could wavefront technology be employed routinely in contact lens practice to the benefit of individual patients and practitioners? As previously mentioned, all contact lenses correct wavefront error to a certain extent. GP lenses correct HOA by replacing the cornea's first surface with a surface that reduces the impact of HOAs in a passive manner. Contact lenses that integrate patient-specific HOA compensation have been demonstrated, and their integration into routine practice is a topic of interest to researchers, contact lens companies, and practitioners. Highly aberrated eyes seem particularly well suited for treatment with these wavefront-guided corrections that reduce both lower-order and higher-order aberrations. However, even as these corrections become available, maintaining varied forms of contact lens correction will remain vital to providing patients with the most appropriate form of correction for their individual needs. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #202.