


Reader and Industry Forum
Scleral Lens Classification: a Different Approach

By Peter E. Wilcox, OD, FOAA
There has been a brisk increase in the number of contact lens specialists who fit GP lenses that exceed patients' horizontal visible iris diameter (HVID). There are also many potential scleral lens fitters who have too many reservations to introduce this lens type to their patients. Most—if not all—current fitters have interesting stories that recount their initial concerns and difficulty with their first scleral lens cases. Many potential fitters may be encouraged to know that an easier point of entry may exist for fitting the growing family of scleral contact lenses.
Current Classification Methods
Simply stated, any contact lens that exceeds the HVID is a “scleral lens.” For those who have avoided these lenses, it may be helpful to note that the incremental increase in diameter is typically linked to an incremental increase in fitting difficulty. Therefore, new fitters may be able to slowly gain experience and confidence by working through the big-bigger-biggest tiers, which in my experience are typically linked with healthy-sicksicker eyes and thus with simplemoderate-difficult fits. In contrast, however, at times you may find it easier-quicker-better to fit a larger-diameter versus a smaller-diameter scleral lens.
Assisting this movement are recent studies in corneal-scleral topography (van der Worp et al, 2010; Jedlicka, 2008), which have reshaped both practitioner thinking and design philosophies within the family of scleral contact lenses. New technologies allow lens design, fitting, analysis, and modifications that were unattainable in the recent past. Over the years, numerous lens diameters, names, and categories have been created to define and describe the variety of lenses that exceed patients' HVID.
TABLE 1
| Scleral Lens Terminology (DeNaeyer, 2011) | ||||
|---|---|---|---|---|
| Alternative Names | Diameter (mm) | Bearing | Tear Reservoir | |
| Corneal | 8.0 to 12.5 | All lens bearing on the cornea | No tear reservoir | |
| Corneo-Scleral | Corneal-Limbal, Semi-Scleral, Limbal | 12.5 to 15.0 | Lenses share bearing on the cornea and the sclera | Limited tear reservoir capacity |
| Full (Scleral) | Haptic | 15.0 to 25.0 | All lens bearing is on the sclera | |
| Mini-Scleral 15.0 to 18.0 | Somewhat limited tear reservoir capacity | |||
| Large-Scleral 18.0 to 25.0 | Almost unlimited tear reservoir capacity | |||
The scleral lens terminology presented by the Scleral Lens Education Society (SLS) (Table 1) was recently published (van der Worp, 2010; DeNaeyer, 2010; DeNaeyer, 2011) with the goal to demystify some of the confusion that has passively evolved over the years. This diameter-to-design-fitting-goals classification system is comprehensive and logical. However, examples of some subtle confusion that I believe are linked to this classification method and that I think could be simplified are:
1. Is a 7.9mm lens a corneal lens?
2. Given that the average corneal diameter of 390 patients was determined to be 11.71mm ± 0.42mm and the total ranges were from 10.70mm to 12.58mm (Rufer et al, 2004) (with personal clinical observations expanding the low and high ranges), then how can a patient who has a 10.7mm HVID and is fit with a 12.4mm lens be labeled as wearing a corneal lens? Additionally, a patient who has a 12.8mm HVID and is fit with a 12.6mm-diameter lens would seem to be wearing a corneal lens and not a cornealscleral lens.
3. Where is the limbus? Different practitioners and instruments have differing opinions on the location of the limbal zone. The limbal reading between different clinicians may differ by 0.1mm to 0.3mm on each edge (0.2mm to 0.6mm total). Optical coherence tomography (OCT) line scans of the circumferential cornealscleral interface reveal a variety of physiological variability within and among various eyes (Figures 1 and 2). I believe that this supports a liberal benchmarking of the various defined lens diameters.

Figure 1. OCT image of the superior limbal zone. When comparing the cross-sectional (top) versus the birds-eye (left) view, the classic “white-to-white” junction is more of a range or zone than a confident spot. Note how the two surfaces feather into each other.
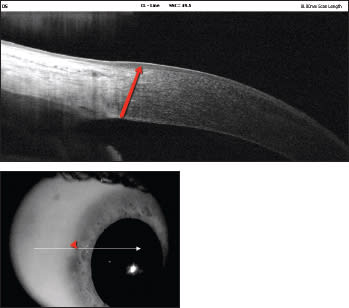
Figure 2. OCT line scan of the nasal limbal zone of the same eye. Note the variability of the interface of the corneal-scleral junction between the vertical and horizontal zones (image 1 versus image 2).
A Different Proposed Method
It may be possible to make these lenses more appealing to the aforementioned fence-sitters by reducing some of the confusion and simplifying the incremental changes in fitting philosophies linked to the various scleral lens types. Table 2 and Figure 3 show proposed alternative terminology. This “3:30” Scleral Lens Classification Table represents an effort to combine the various HVIDs as well as the design intentions of the family of scleral lenses. Because the 2mm+ range of HVIDs (Rufer et al, 2004) needs to be considered in the lens selection and design/fitting, individual patients' HVIDs serve as the foundation for the new nomenclature.
TABLE 2
| “3:30” Scleral Lens Classification Table | |||||
|---|---|---|---|---|---|
| Abbreviation | Diameter | Bearing | Tear Reservoir | ||
| Corneal Lens | C | Up to HVID | All on cornea | Thin film | |
| Limbal Lens | L | Equal to HVID | All on cornea | Thin film | |
| Corneal-Scleral | CS | 0.0mm to 3.0mm greater than HVID | Shared bearing on cornea and sclera | Thin film to hundreds of microns | |
| Semi-Scleral | SS | 3.1mm to 6.0mm greater than HVID | All bearing on sclera | Minimal to hundreds of microns | |
| Scleral Lens | S | 6.1mm+ greater than HVID | All bearing on sclera | Hundreds to a thousand (±) microns | |

Figure 3. The “3:30” Scleral Lens Clock.
Under the proposed new classification system, a corneal (C) lens is any lens diameter that does not exceed a patient's HVID. A limbal (L) lens closely matches a patient's HVID (included for literature completeness). A cornealscleral (CS) lens has an overall diameter (OAD) that is 0.0mm to 3.0mm greater than a patient's HVID. A semi-scleral (SS) lens has a diameter that is 3.1mm to 6.0mm greater than a patient's HVID. Finally, a scleral (S) lens has a diameter that is 6.1mm or more greater than a patient's HVID.
Neither Table 1 nor Table 2 is without occasional confusion or error, but I believe that in the interest of simplifying a field of increasing players (both practitioners/designers and manufacturers), the rule of “less is more” applies. In my experience, simplification in both design and practitioner/patient communication is a major key to a successful practice as well as successful marketing. I believe that the “3:30” Scleral Lens Clock has a simplicity that makes it a good tool for patient education.
A Closer Look at the Clock
The “3:30” Scleral Lens Classification Table clarifies the “clock” and notes what I have found are the incremental challenges with increasing lens diameter. The “3:30” is the “time” on the clock, in which the “little hand” (smaller-OAD lenses) is on the 3 o’clock hour and the “big hand” (junction between the bigger and biggest lenses) is on the 6 o’clock hour. The green, yellow, and red colors are designed to serve as visual indicators to both practitioners and patients that as the lens design increases in diameter, so may the complexity of the fit, the possible complications of the given eye, and the expenses borne by the practitioner/patient. Because the 3mm and 6mm benchmarks are guidelines, it is arguable that a better image would have a blending of the color changes, which would acknowledge the exceptions in design goals and realities between the inflection points. However, this was not adopted to remain loyal to the clock's intended simplicity.
0mm to 3mm > HVID = Corneal-Scleral Lenses = Green I have found that there are many more applications for CS lenses than for SS or S lenses. Fitters just entering this arena may be comforted that the dual-bearing on the cornea and the sclera incorporates many corneal GP fitting philosophies and logic. The lens simply extends onto the conjunctival surface, which provides superior lens stability, centration, and comfort. I used green to indicate a non-or partially diseased eye, a simpler fitting process, and usually a lower cost.
In addition, there is simply not enough room to do much else but share the bearing of the lens on the cornea when there is only 1.5mm or less of landing area on the sclera (1.5mm on “each side”). Vaulting of the cornea and limbus thus requires a total OAD that is typically greater than the HVID + 3.0mm, which brings us to the next scleral lens category.
3.1mm to 6.0mm > HVID = Semi-Scleral Lenses = Yellow Semi-scleral lenses (also known as mini-scleral lenses) are designed to vault the cornea. Patients fit with such lenses may have a compromised cornea from diseases or conditions such as keratoconus, pellucid marginal degeneration recurrent corneal erosions, or dry eye or from undesired surgical outcomes. The well of the lens is filled with preservative-free saline, which bathes and protects the cornea while helping to provide superior vision.
I used yellow to signify a more difficult fitting process that is different from conventional corneal GP logic. The lens must be designed to vault the cornea as well as the limbus while gently resting on the sclera with such minimal pressure that the fine conjunctival vessels maintain their patency.
6.1mm to 12.0mm > HVID = Scleral Lenses = Red Combining the previously mentioned average HVID of 11.71mm ±0.42mm with these values of 6.1mm to 12.0mm means that a scleral lens under this classification system would have OADs ranging from 17.29mm to 18.13mm. Though the criteria to be a true scleral lens may be satisfied at smaller diameters than these, this satisfies the intention of a communal understanding. I have found that there are vastly different fitting challenges, presenting patient/corneal complications, fitting considerations, and greater expertise, required time, and materials cost associated with these largest in the family of scleral lenses.
The greater scleral asymmetry from the variable insertion of the recti muscles (van der Worp et al, 2010), the larger haptic and affiliated vessel blanching, the significantly greater volume of captured saline, and the greater difficulty of application and removal may require a significantly greater level of commitment by both practitioner and patient. Red denotes these factors to both patients and to professionals offering this option.
Summary
Where does this lead? I believe the Clock, with its three familiar “traffic light” colors and the two numbers 3 and 6, distills the frequently confusing collective of information surrounding the family of scleral lenses. With a wink and a nod to excuse the variability among patients, along with the unavoidable exceptions to the rule, we can serve to unite a growing marketplace while acknowledging the complexity and seriousness associated with many of those who benefit from these larger-than-HVID lenses. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #202.
| A graduate of the University of Alabama at Birmingham School of Optometry, Dr. Wilcox completed a Primary Care residency at Pennsylvania College of Optometry. He is in private practice in Hayes, Va. He can be reached at doc@wilcoxeye.com. |