


Contact Lens Case Reports
Corneal Reshaping for Myopia Control in an Astigmatic Patient


BY PATRICK J. CAROLINE, FAAO, & MARK P. ANDRÉ, FAAO
Our patient was a 9-year-old male referred to our clinic for myopia control via orthokeratology/corneal reshaping. His spectacle Rx was right eye: −4.00 −0.50 × 170 and left eye: −4.00 −0.50 × 10 with visual acuities of 20/15. Corneal mapping and simulated keratometry showed 0.87D of corneal astigmatism OD and 1.00D OS (Figure 1). The patient was subsequently fitted with Paragon CRT (Paragon Vision Science) lenses with a prescription of 8.5mm base curve, 0.550 return zone depth (RZD), and −34 landing zone angle (LZA). Post-wear corneal topography maps showed well-centered treatment zones, but after one month of overnight lens wear the patient’s uncorrected visual acuities were between 20/25 and 20/30.
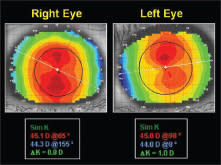
Figure 1. The patient’s pre-fitting corneal mapping showing approximately 1.00D of corneal astigmatism.
Evaluation of the patient’s corneal topography (and lens parameters) using the new CRT Fitting Software showed an appropriate apical clearance of 7 microns OD (Figure 2) and 7.4 microns OS. The “target” in corneal reshaping is typically between 5 microns and 10 microns.
The topographical changes that take place in overnight corneal reshaping result from fluid forces beneath the contact lens. Therefore, a key ingredient to this process is that every corneal reshaping lens must “land” peripherally 360 degrees around the cornea, which lessens the rapid escape of the fluid forces. In this case, the software revealed that the patient’s inability to achieve full correction may have been due to an excessive amount of peripheral lens clearance along his steeper vertical meridian.
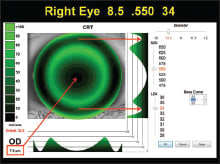
Figure 2. Software simulation of the traditional CRT lens on the patient’s right eye. Note the peripheral landing of the lens along the horizontal meridian and the excessive clearance along the vertical meridian.
A Change in Design
We ultimately fitted the patient with the Paragon CRT Dual Axis lens design that incorporates two different return zone depths: a shallower return zone to align with the flat corneal meridian, and a deeper return zone to align with the steeper corneal meridian. The Dual Axis design allows the lens to better maintain the necessary post-lens fluid forces for improved centration and enhanced treatment. Figure 3 shows how the individual lens parameters can be adjusted within the fitting software to optimize the simulated fluorescein and tear film profile patterns.
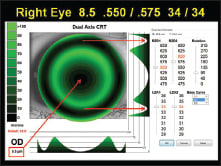
Figure 3. Software simulation of the Dual Axis lens design. Note the improved relationship of the lens along the vertical meridian.
One week after initiating wear of the Dual Axis lenses, the patient’s uncorrected visual acuities were stable at 20/15. CLS
Patrick Caroline is an associate professor of optometry at Pacific University. He is also a consultant to Paragon Vision Sciences. Mark André is an associate professor of optometry at Pacific University. He is also a consultant for CooperVision.