


Reader and Industry Forum
Mixed Astigmatism Treated With a Dual-Toric Ortho-k Design

By Antonio Calossi, DIP OPTOM, FBCLA, FIACLE
Using orthokeratology to correct astigmatism remains a debated topic. In most cases, excessive corneal toricity and astigmatism that is greater than the spherical component of the refractive error are considered contraindications to orthokeratology.
Here I present a case of mixed astigmatism in a patient who was intolerant to traditional toric contact lenses and was strongly motivated to try overnight orthokeratology.
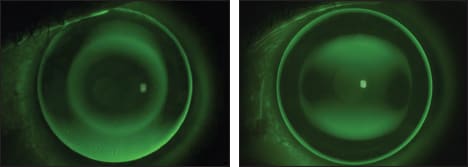
Figure 1. Fluorescein patterns showing the different alignment of a spherical ESA (left) and the dual-toric ESA (right).
Case History
The patient was a 44-year-old woman with a refraction of: OD +1.00 −2.00 × 180 (20/16), OS +1.25 −2.25 × 180 (20/16). Uncorrected distance visual acuity (UDVA) was OD 20/40, OS 20/50, OU 20/35. Near point was 40cm. Corneal topography showed a slightly asymmetric toricity. Biomicroscopic examination showed no significant signs, but a minor dry eye.
For this challenging case, I designed a hexacurve, dual-toric, reverse geometry (ESA bitorica) lens in which the back surface had two different toricities: one for the alignment zone and the other for the optical zone. The vertical meridian was steeper than the horizontal meridian in the midperipheral alignment zone, and vice versa in the optical zone.
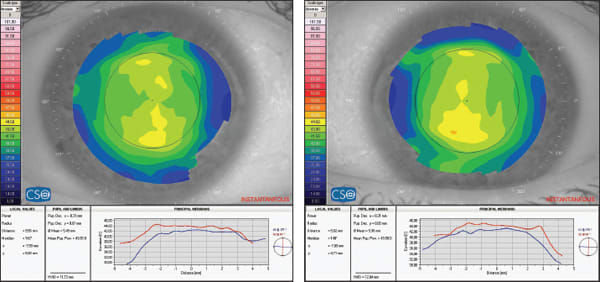
Figure 2. Pre-treatment corneal topography and curvature graph of the right and left eyes.
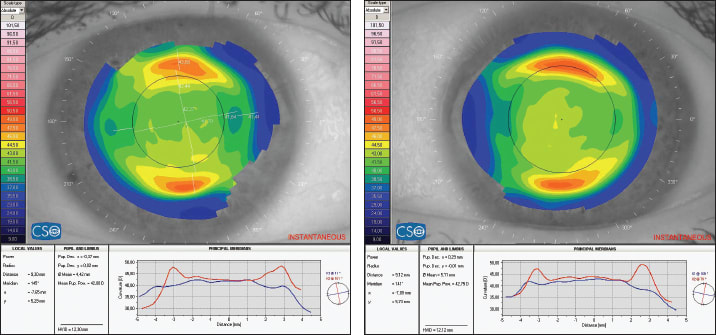
Figure 3. Post-treatment corneal topography and curvature graph of the right and left eyes.
The lenses were manufactured in a fluorosilicone acrylate material (Boston XO, Bausch + Lomb), Dk 100, for overnight wear. Figure 1a shows the fluorescein pattern of a spherical ortho-k ESA lens on this patient, and Figure 1b shows the same eye with the dual-toric design.
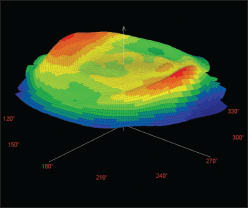
Figure 4. The 3D representation of corneal curvature shows the steepening of the horizontal meridian and the flattening of the vertical meridian.
Results
After one week of overnight wear, corneal topography showed a reduction of central toricity, with a homogeneous optical zone. UDVA was OD 20/16, OS 20/25, OU 20/16, and her refraction was OD +0.50 −0.75 × 10 (20/16), OS −0.25 −1.00 × 5 (20/16). Near point had moved to 26cm. Without any correction, the patient reported good quality of vision both day and night.
After three months, the patient’s unaided vision continued to be excellent for both distance and near. UDVA was OD 20/16, OS 20/23, OU 20/13, and her refraction was OD +0.50 −0.50 × 10 (20/16), OS +0.25 −1.00 × 5 (20/16).
After one-and-a-half years, her unaided vision was still good and she continued to not need spectacles. During this follow-up period, no adverse reactions were observed. Figure 2 shows her pre-treatment corneal topography, and Figure 3 shows her post-treatment topography. Figure 4 shows the steepening of the horizontal meridian and the flattening of the vertical meridian.
Conclusion
Although excessive corneal toricity and astigmatism that is greater than the spherical component of the refractive error are considered contraindications to orthokeratology, the use of a dual-toric, reverse geometry lens design allowed a satisfactory correction in a case that was apparently contraindicated to this method of treatment. CLS
Antonio Calossi, Optometrist, FBCLA, FIACLE, practices in Certaldo (Florence), Italy and is a lecturer of Contact Lenses at the department of Optics and Optometry at the University of Florence, Italy. As an independent consultant, he is involved in R&D programs in the fields of ocular diagnosis, corneal topography, aberrometry, refractive surgery, contact lenses, and orthokeratology. He is a consultant or advisor to Alcon Ciba Vision, CSO, Esavision, Nidek, and TS lenti a contatto, and he holds a patent on the ESA Ortho-K design. He may be reached at calossi@ortho-k.it.