


May 2013 Online Photo Diagnosis
By William Townsend, OD, FAAO
COURTESY OF JANET L. TOWNSEND, OD
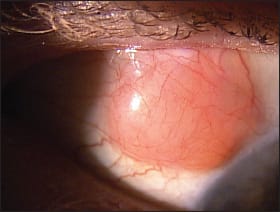
This 59-year-old female presented to our office complaining of foreign body sensation of the right upper eyelid. She noted and was able to palpate a mass in the right upper lid. She denied trauma. Her general health history included Sjögren’s syndrome, hypertension, and rheumatoid arthritis. She had an ocular history of corneal epithelial basement membrane dystrophy, recurrent corneal erosion, hypertensive retinopathy, herpes zoster with recurrent keratitis and uveitis OD, and cataract surgery OD.
Gross external examination revealed a 12mm × 12mm × 4mm elevated, salmon-colored lesion on the superior, temporal bulbar conjunctiva. The lesion was firmly attached to the underlying tissue. Other findings included multiple punctate scarring of the right cornea, pseudophakia OD, and deep, quiet anterior chambers OD and OS.
Differential diagnosis of surface conjunctival lesions includes papilloma, lymphoma, squamous cell carcinoma, inflammatory pyogenic granuloma, and amelanotic melanoma.1 We started the patient on prednisolone acetate and referred her to her primary care provider for systemic workup. We also referred her to an anterior segment specialist for possible biopsy or imaging.
The lesion was subsequently excised and sent to pathology for evaluation. It was ultimately identified as a small B-cell follicular lymphoma.
Lymphoma is a form of cancer arising from B and T lymphocytes. It is classified as either Hodgkin or Non-Hodgkin lymphoma. Hodgkin lymphoma is characterized by orderly spread from one lymph group to another and by the presence of multinucleated Reed–Sternberg cells. Non-Hodgkin lymphoma is any lymphoma that does not meet the criteria for Hodgkin disease. Lymphoma typically presents as a solid tumor of lymphoid cells, often arising from a lymph tissue, i.e., lymph nodes, the spleen, the liver, and blood. Extranodal tumors, i.e., not arising from a lymph node, develop in the brain, bowels, bone and other tissues including the eye and ocular adnexae.2,3
Our patient was diagnosed with a B cell follicular lymphoma of the ocular adnexa. Ocular adnexal lymphomas (OALs) comprise 1 percent of non-Hodgkin lymphomas and 5 percent to 15 percent of extranodal lymphomas. Their incidence is increasing, and they are thought to develop after a "triggering incident," which may include chronic inflammation, persistent infection, or autoimmune disease. Chronic antigenic stimulation predisposes the site for development of lymphoma. Chronic infection is also a potential trigger; DNA from Chlamydia psittaci, the intracellular obligate parasite that causes psittacosis, has been detected in 75 percent of patients who have conjunctival lymphomas. Humans acquire the infection through exposure to infected birds, cats, and other animals.4,5
In this patient’s case, possible predisposing factors included Sjögren’s syndrome, rheumatoid arthritis, and chronic, recurrent herpes zoster infection/inflammation. The prognosis for conjunctival B cell lymphoma is excellent, with a five-year overall survival rate of 93 percent.
References:
1. Shields J.A., Shields CL. Review of Ophthalmic Tumors. Oncology Service, Wills Eye institute, Philadelphia February 2013. accessed 14 May 2013 retrieved from nyee.edu/pdf/okap-shields.pdf.
2. Lymphoma wikipedia.org/wiki/15 May 2013 accessed 15 May 2013
3. Woolf D.K., Ahmed M., Plowman P.N. Primary Lymphoma of the Ocular Adnexa (Orbital Lymphoma) and Primary Intraocular Lymphoma. Clinical Oncology 24 (2012) 339-344
4. Coupland SE Molecular pathology of lymphoma. Eye (2013) 27, 180–189.
5. Volmer L. The diagnosis and management of ocular lymphoma. Optometry and Vision Science, Vol. 90, No. 2, February 2013