


Custom Scleral Case
Customized Scleral Fit in a Case of Keratoconus
Scleral obstacles and a limited timeframe made this case particularly challenging—and very rewarding.
By Luciano Bastos & Marcelo Bittencourt, MD

|
Mr. Bastos is the director and clinical instructor of specialty contact lenses at the Instituto de Olhos Dr. Saul Bastos (IOSB) and is the director and specialty lens consultant of Ultralentes, a small laboratory specializing in GP and scleral lens designs in Porto Alegre, RS, Brazil. He has lectured at ophthalmology meetings in Brazil as a specialist on the subject of contact lenses. |

|
Dr. Bittencourt is the clinical director at IOSB and also works as a consultant for the ophthalmology department of Presidente Vargas Hospital in Porto Alegre, Brazil. He is also affiliated with to the Banco de Olhos de Porto Alegre Hospital. |
In some cases of corneal disease, a scleral lens fitting is the only option that can save a patient from undergoing a corneal transplant. This article describes just such a patient from Sao Paulo, Brazil, who came to our clinic at Instituto de Olhos Dr. Saul Bastos (IOSB) in southern Brazil. He had bilateral keratoconus, dry eye, and pingueculae as well as a long history of failures and complications that arose from previous treatments and contact lens fittings. He was about to undergo a corneal transplant, but then heard about our work at IOSB; he told us that we were his last hope.
It is a real challenge when a patient says something like that, but we were determined to achieve a successful fit.
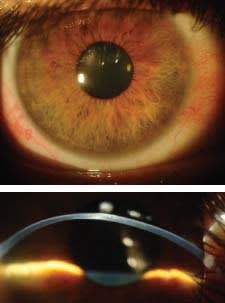
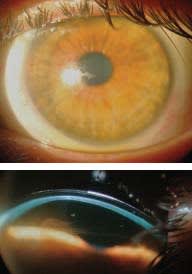
Figure 1. Right eye front view (note redness) and slit lamp 45° cross-section view, turned right.
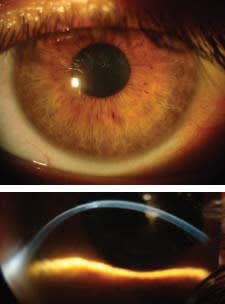
Figure 2. Left eye front view and slit lamp 45° cross-section view, turned right.
Case Report
Our patient was a 32-year-old male engineer who had bilateral keratoconus. He underwent intrastromal ring implants, a subsequent procedure to extract the rings as he had an extrusion of one segment, and then corneal crosslinking (CXL). None of these procedures improved his visual acuity.
He had visited several practitioners in Brazil and in the United States, where he lived for a year studying abroad. While in the United States, he was fitted with hybrid lenses, which he initially was able to wear for 12 hours to 13 hours a day. He developed bilateral redness after several months of wear, after which wearing time decreased rapidly until he could no longer tolerate the hybrid lenses. He also reported a burning sensation during lens wear.
Once he returned to Brazil he was fitted with Rose K2 (Menicon/Blanchard) lenses in both eyes, which he could wear for five hours to six hours daily before redness would appear. The patient’s eyes were very sensitive and developed redness occasionally and spontaneously, to which we attributed lacrimal deficiency as a probable cause.
Initial Evaluation
At the first examination, we measured a tear breakup time of 5 seconds to 6 seconds, and we also observed a nasal pinguecula OD and OS. We had instructed him to not wear his GP lenses for four days prior to the examination to ensure that they did not influence the corneal topography. Despite the CXL procedure and the fact that at this age the cornea is more stable, keratoconic eyes commonly have an altered corneal hysteresis and a weaker biomechanical resistance.
His K readings were OD 46.62 x 49.12 @ 135 and OS 52.12 x 45.87 @ 57. Rx readings were OD –6.25 –2.75 x 118 and OS –8.00 –4.12 x 48. His uncorrected visual acuity was OD 20/80 and OS 20/200.
Figure 1 shows the front and 45-degree cross-section views of his cornea OD, and Figure 2 shows both views OS. The patient was prone to conjunctival hyperemia, which he reported began about one year after undergoing the CXL procedure a few years previously. These images show a less irregular surface OD and a more prolate, ectatic cornea OS.
We obtained both corneal topography and anterior segment tomography (Pentacam, Oculus) for both eyes. The Pentacam exam provided data across 12mm of the cornea and also supplied the limbus-to-limbus measurement (Figure 3). Figure 4 shows the anterior sagittal curvature topography. We’ve found that the larger corneal area measured by the Pentacam instrument is helpful in choosing initial scleral diagnostic lenses as compared to using traditional topography, which measures only 8mm to 9mm of the cornea.

Figure 3. Limbus-to-limbus measurement.
Initial Diagnostic Lens Fitting
We first attempted to fit corneal GP lenses with the Ultracone Nipple design manufactured by Ultralentes in Brazil. This design has an overall diameter ranging from 8.2mm to 9.2mm and features a progressive aspheric transition zone. The patient asked us to try this type of lens first as he was wearing similar lenses and this was his only pair. We achieved a successful fit with this GP lens design (Figure 5), but note the staining with fluorescein due to tear film instability. The initial fluorescein pattern made it appear that the fit was fine, but we were concerned that this would change after a few hours of wear and that dryness symptoms would develop.
By contrast, scleral lenses would provide constant corneal hydration for the entire duration of lens wear. We therefore recommended trying scleral lenses due to his tear film instability, which we believed would again cause discomfort after continued wear of the corneal lenses. The patient agreed to try scleral lenses, and we moved forward with an initial fitting.
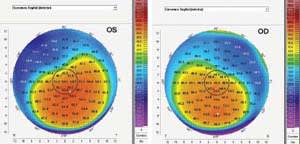
Figure 4. Anterior sagittal curvature along 12.0mm of both corneas.
Switching to a Scleral Design
We used the topography maps generated by the Pentacam as well as corneal assessment using the slit lamp cross-section view to determine the initial trial scleral lenses. We observed that the right eye had a less irregular surface overall compared with the left eye. Using this information, it was relatively easy to determine the correct scleral lens design, base curve, diameter, and sagittal height for the diagnositc contact lenses. We chose the Scleral Bastos (Ultralentes) design for both eyes with parameters of OD 43.00D base curve radius (BCR), 18.5mm overall diameter (OAD), 5.701 Sag, –5.00D power, Ultraflat Scleral Bastos (SB) design and OS 47.00D x 43.00D BCR, 18.0mm OAD, 5.791 Sag, –6.00D power, Ultracone SB design. Figure 6 shows the fit of these initial lenses.
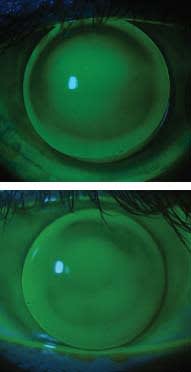
Figure 5. OD and OS fit with Ultracone Nipple.
The Ultraflat SB design OD provided good alignment with good corneal and limbal clearance and even bearing on the sclera. This design has a larger optical zone compared to other scleral lenses, with applications ranging from flatter, post-surgical corneas to mild-to-moderate corneal ectasias. The Ultracone SB design has two base curves, and because the optical zone is also larger than in other scleral lens designs, it allows even greater sagittal height values than usual for scleral lenses.
Both designs have what we call Spline Wave Technology, which allows tear or liquid lens reservoir exchange. We believe that tear exchange plays an important role in providing sufficient oxygen transmission to the cornea, thereby avoiding hypoxia due to the large area covered by the lens and the fact that scleral lenses are thicker compared to corneal GP lenses. Oxygen transmissibility is inversely proportional to lens thickness, so we believe that if the lens allows even a slow fluid exchange, this is good for the overall physiological health of the ocular surface, especially the cornea. A trapped liquid reservoir in a sealed scleral lens fit may exhaust the oxygen supply, even when using hyper-Dk lens materials. This may vary from case to case and from one scleral lens design to another.

Figures 6a and b. Slit lamp front view and cross-section view, turned right, Ultraflat SB (OD).
Figures 6c and d. Slit lamp front view and cross-section view, turned right, Ultracone SB (OS).
While corneal clearance was adequate, we determined that minor modifications could be made to improve clearance at the limbus. Both lenses demonstrated slow but effective lacrimal exchange. Figure 7 shows the fluorescein patterns after five to seven minutes, with the fluorescein instilled over the trial lenses using a lubricated fluorescein strip.
Arriving at the Final Scleral Lens Design
Obtaining the desired corneal and limbal clearance was not a problem—we simply planned a larger optical zone with a larger transition. The final scleral lens parameters were OD 42.75D (7.89mm) BCR, 18.8mm OAD, 5.913 Sag, –3.50D power, 125 Dk and OS 46.50D x 42.00D (7.26mm x 8.03mm) BCR, 18.8mm OAD, –6.50D power, 5.943 Sag, 125 Dk. Best-corrected visual acuity (BCVA) with the sclerals was 20/20 OD and 20/25 OS.
Note that despite a flatter base curve, the sagittal height value was increased by the changes at the optical zone and overall diameter to achieve a better alignment and to guarantee clearance at the limbus. We were able to dispense these scleral lenses and educate the patient on their application, removal, handling, and cleaning. The lenses seemed satisfactory for the moment, but we did notice what seemed to be mild haptic compression nasally at the pinguecula OD and OS, so we needed to re-evaluate the fit.
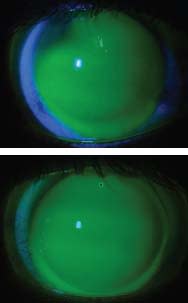
Figure 7. Fluroescein patterns of trial lenses OD and OS.
Managing Unexpected Difficulties
As we had only five days to resolve fitting issues because the patient had to return home for work, we asked him to wear his sclerals for an entire day and then saw him after nine hours of continued wear. This is sufficient wear time for evaluating initial signs of any obvious complications. We observed that the patient had localized redness exactly where the pinguecula was located in both eyes (Figure 8). The patient reported comfort with both lenses despite the redness. However, he was concerned because when he had developed redness with his previous lenses it was across the entire eye, and with the scleral lenses it was very localized.
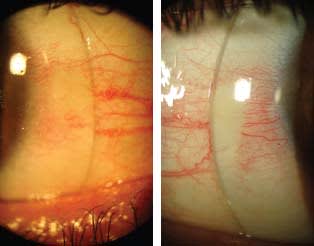
Figure 8. Nasal sclera with pinguecula OD and OS.
Managing the Lens Fit Over the Pingueculae We carefully examined the nasal conjunctiva of both eyes to determine the elevation of each pinguecula and to gain a better understanding of how they were affecting the lens fit. Figure 9 shows a slit lamp cross-section view of both nasal sclera. It is important to mention that sometimes the front slit lamp view alone simply will not provide a true idea of what is happening under the lens or even at the sclera. You can use the slit lamp cross-section white beam while the patient turns his eyes temporally to observe and estimate the conjunctival elevation.
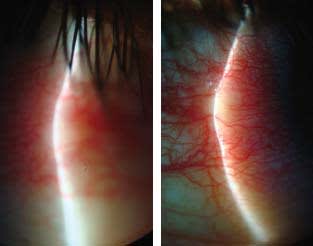
Figure 9. Cross-section view of pinguecula OD and OS.
Figure 10 shows another way in which I attempted to determine the height of the pinguecula OS, which in this case was the more severe. The image was taken with a special macro lens adjusted to obtain a perspective view of the area beyond the cornea from the point of view of the apex.
At this time I remembered an article from Gregory W. DeNaeyer, OD, FAAO, in which he discussed avoiding scleral obstacles by going around them (De-Naeyer, 2012). So we used the images we had obtained of the scleral and conjunctival irregularities to determine the best way to overcome these obstacles, whether by working around them or over them without compromising the ideal lens fit. Unfortunately, there is no technology available to provide this information, so you need to go by what you can see. However, it is possible to estimate what is necessary based on the images that you take and the scleral lens design if you know the exact parameters.

Figure 10. Pinguecula OS from a different viewpoint in an attempt to measure its contour.
We decided to make a few adjustments to the lenses at the laboratory. The idea was to make new lenses with a non-rotationally symmetrical haptic that would overcome and gently contour the pingueculae without constricting them. It is important to note that without the help of our team at IOSB and also from the Ultralentes lab, this task would never have been possible. It is important to maintain a good relationship with your lab technicians, as a large part of the fitting success will be contributed by them. Figure 11 shows the modifications to the lens OS.
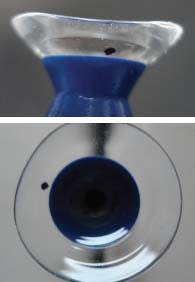
Figure 11. Modified scleral lens OS.
Testing the Customized Haptic Scleral Lenses The patient received his modified scleral lenses at the end of day 4 and wore them for seven hours the next day, coming in for a final follow-up visit before going to the airport. He presented with a better conjunctival response, both lenses appeared to fit better.
The scleral lenses provided better vision, great comfort, and his hyperemia was significantly reduced. Both lenses have minimal movement and allow oxygen exchange through both the high-permeable material and the spontaneous fluid exchange. Figure 12 shows the modified lenses contouring the pingueculae on day 5 after seven hours of continued wear. His eyes were still a bit red from the day before on this final day.
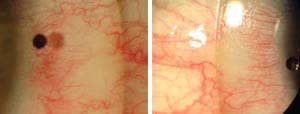
Figure 12. Scleral lens edge contouring nasal pinguecula, OD and OS.
The final lenses were acceptable to the patient. We instructed him to slowly increase his wearing time and to return for a follow-up visit in two weeks.
Follow-up Evaluation
The patient came for a follow-up visit 15 days after the lens dispensing visit. Figure 13 shows the appearance of the lenses through the slit lamp. He reported successfully wearing his lenses for about 14 hours a day; he also reported that the right eye still developed slight redness with wear that would disappear 30 minutes to 45 minutes after lens removal. He further mentioned that he was not instilling the preservative-free artificial tears that we had prescribed—he said that he used the lubricant only when he thought he would need it. We reinforced the need of using it more often even if he thought that it was not necessary.

Figure 13. Slit lamp front view after 15 days of lens wear, OD and OS.
Three-Month Follow up After 90 days of wear, the patient was seen by his practitioner in Sao Paulo, who contacted us to assure us that the patient was doing well with his sclerals and that the modifications we had made to the lenses were helping to prevent complications. The practitioner also pointed out that there was an overcorrection OS of 0.25D, which the patient did not complain about.
Eight-Month Follow up After eight months, the patient was still successful and happy with his scleral lenses and wanted to have an additional pair. The challenge this time was to manufacture an identical or even better pair of scleral lenses to maintain the given results. The new lenses provided similar comfort and visual acuity. Figure 14 shows their appearance through the slit lamp.

Figure 14. New scleral lenses OD and OS.
Conclusion
This case was especially challenging because we had only a short span of time to design contact lenses that worked for this patient. We did not know that he had scleral obstacles in the form of pingueculae before the initial evaluation because we had access only to his topography and history before his visit.
But we have found that it is possible to overcome most scleral obstacles when fitting scleral lenses, although significant modifications to the lens design may be necessary to customize a lens that will allow a proper fit. In cases like this, you need to create a lens based on what you see, observing the ocular surface from different angles to help in determining what would be the best possible lens design.
It is also important to adjust the fees that you charge. Challenging cases such as the one described here can be time consuming, so you deserve to be paid accordingly. Patients are usually very willing to pay a higher fee when you help them avoid a corneal transplant with a well-fitted contact lens. CLS
For references, please visit www.clspectrum.com/references. asp and click on document #214.