


MINI-SCLERAL FITTING
Mini-Scleral Lens Fitting and Problem Solving
A look at how to overcome some common hurdles when fitting mini-scleral lenses.
By Bezalel Schendowich, OD, FIACLE
Over the past several years, I have had the opportunity to use what I believe is one of the world’s outstanding contact lens designs in helping many of my patients who have distorted corneae regain sight.
The particular lens I refer to is one of the growing number of mini-scleral lens designs marketed today. When fit correctly on appropriate eyes, patients can profit from long hours of comfortable wear and gain the potential for greatly improved visual acuity.
The promise of scleral lenses is multifaceted. When managing seasoned corneal GP contact lens wearers with years’ experience, and especially those who have difficult-to-fit corneal surfaces, contact lens fitters may hear complaints ranging from subtle irritation to outright anguish.
This mini-scleral lens markets itself: comfort is vastly improved from the first moment, the lenses do not fall out, they do not trap foreign bodies, and they will not dislodge or travel around on the ocular surface. From their size alone, they are easier to find if dropped, and their greater mass renders them much less breakable.
To be fair, life with this amazing lens design is not all a bed of roses. Not every patient is comfortable with the size of the lens. Not every prospective candidate can fit the additional aspects of this lens’ care routine into their daily schedule. And, the fact that the lens is more expensive compared to other lens designs that patients may have used in the past can be rather dissuasive. Even though the fitting process is pretty much straightforward, the learning curve can seem to be rather long; it depends greatly on the patients and on the eyes with which you work. In my case, I believe—and my laboratories contend—that I am “pushing the envelope” with almost every patient. Nonetheless, I continue to work with my patients and this mini-scleral design because of the lens’ inherent strengths.
Achieving an Ideal Fit
The fitting paradigm for these mini-scleral lenses begins with their apparent sagittal height (sag) over the cornea. According to the various fitting guides, this should remain between 150 to 250 microns after the lens settles (Figure 1). This sag is high enough to protect the cornea from abrasion due to lens bearing while low enough to reduce the chance of engendering large bubbles. These bubbles (Figure 2), when they occur, interfere with visual acuity and also raise the risk of abrasion because the air that comprises them is dry relative to the fluid in the chamber and can rub the corneal epithelium in a way similar to that of a solid foreign body.

Figure 1. Proper sagittal height of a mini-scleral lens over the cornea.
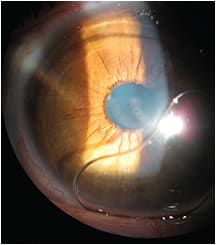
Figure 2. Large bubble under a mini-scleral lens resulting from too high a vault.
Fitting continues with the area over the limbus, where clearance must also be neither too high nor too low. If the sag over the limbus is too great, conjunctival decompensation can result. The negative pressure gradient can draw loose conjunctiva under the lens in a billowing formation (Figure 3). It is still an open question as to whether this billowing, also called conjunctival prolapse, is a safe or a pathologic change. On the other hand, if the sag over the limbus is too low, pressure on the limbal stem cells can cause injection, corneal inflammation, irritation, and perhaps strangulation of the limbal stem cells. The resulting pathology compromises corneal epithelial regeneration. Other changes caused by limbal compression include opacification of the cornea near the limbus and neovascularization.
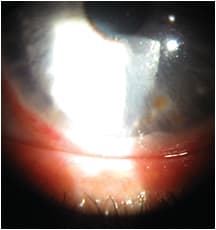
Figure 3. Excessive clearance over the limbus can draw loose conjunctiva up under the lens.
Finally, careful attention must be paid to the landing zone. The edge of the lens should ride parallel to the surface of the conjunctiva. A deep edge will cause blood vessel blanching and post-removal reflex injection. An edge with too high a lift will not be comfortable. Good lens geometry will allow the conjunctiva and conjunctival blood vessels to be easily wiggled under the edge of the lens. Fluorescein instilled outside of the lens should be able to flow under the lens with several blinks. A lens designed in this way, coupled with correct blinking habits, will ensure sufficient exchange of intracameral fluid to prevent a toxic eye condition, and it will allow the eye to remain white and quiet through the day.
Troubleshooting Mini-Scleral Fitting Problems
Toxic Eye The most colorful expression of a poor contact lens-to-eye relationship is a toxic eye (Figure 4), which results from an extremely tight lens haptic. The conjunctiva appears both white and red in concentric bands. The white represents the pressure of the lens haptic zone on the landing zone of the sclera, which compresses the blood vessels. The red areas both around and within this band of blanching emphasize the obstructive effect that the lens pressure exerts on the blood vessels.

Figure 4. A toxic eye resulting from a mini-scleral lens haptic that is too tight.
Because the lens is so tight on the eye, there will be no exchange of post-lens fluid, and metabolic toxins will accumulate in the pre-corneal cavity. These moieties affect the epithelium and can attach to the posterior lens surface, building up to the thickness of a film that will cloud vision. There is also a tendency for the fluid held by the lens to become cloudy.
My approach to treating toxic eye syndrome is built upon four principles: 1) edge configuration, 2) saline exchange during the day, 3) full blinking, and 4) thorough cleaning.
Edge Configuration There are three possible edge relationships to the conjunctiva over the scleral landing zone: 1) low/indenting/blanching, 2) high, and 3) parallel.
Obviously, a parallel fitting relationship is healthier for the tissue compared to a low or blanching edge, and it should be more comfortable to the eyelid margins compared to a high edge configuration. For the purpose of better fluid circulation, a slightly higher than parallel edge would be the best of all. This edge design, along with full blinking, would allow for a gentle tilt-pump-exchange of tears with the saline and debris that fills the tear reservoir with time.
Saline Exchange During the Day Many fitters suggest as a rule that their scleral patients remove their lenses and refresh the saline bath after each four or so hours of wear. Such fitters have most likely concluded that it is necessary to ritualize the change of saline after observing that many of their patients exhibit tight lenses. They have found that it is easier to break the seal of the lens to the eye earlier in the wearing day and, additionally, that the eye will benefit from the refreshed solution in many ways.
Full Blinking Full and competent blinking is important for the health of the eye, the condition of both surfaces of the contact lens, clarity of vision, comfort of lens wear, and length of the lens wearing day. It is my contention that a best-fit lens requires a full blink to generate a very mild pumping action, resulting in an exchange of fluids behind the lens. Those patients who succeed with their scleral lenses, like those who wear corneal lenses, have learned how to accomplish this exchange. Those who initially succeed and gradually lose their white and comfortable eyes are probably becoming lazy about blinking.
Thorough Cleaning A major pitfall for many scleral wearers, as well as with many other contact lens designs, is thorough cleaning and protein removal. The most interesting aspect of scleral lens deposition might well be the buildup of protein on the inside surface of the lens even with the constant fluid bath.
I try to teach my patients to use their little finger to rub inside the bowl of the lens; others suggest a cotton swab moistened with lens cleaning solution. I have found that a weekly soak in full-strength peroxide-based contact lens disinfectant (without neutralizer or disk) leaves lenses crystal clear. To accomplish this, instruct patients to clean the lenses according to the daily protocol upon removal and then to place them into a deep well case with the peroxide solution. In the morning, patients should empty the lenses out onto a clean soft cloth, dry them with a tissue, and condition them prior to application.
Loose Floppy Conjunctiva Some patients present with motile conjunctiva. This can be problematic both under and around the perimeter of a scleral lens. As mentioned previously, when the midperipheral sag (above the limbus) is too high, loose conjunctiva can billow up under the corneal segment of the lens. When the bulbar conjunctiva around the edge of the lens is loose and nearly chemotic, it can bunch and enclose the edge of the lens, resulting in pain and minor trauma to the conjunctiva when the lens is removed. My experience has not demonstrated a good solution to the peripheral conjunctiva problem with the mini-scleral lens design. I suppose that a full scleral lens with an evenly fitted haptic will comfortably compress the conjunctiva without bunching it.
The Perplexing Problem of Residual Cylinder From time to time, after trialing lenses and working through the fitting calculations required for changes in the midperiphery or edge, vision with the ordered lens in situ is poor. The lens fit, position, and movement all seem optimal, but the patient still complains of poor vision. Over-refraction with cylinders shows 1.00D to 2.00D of uncorrected astigmatism. Where does it come from? How should we handle it?
Part of the answer to this question may well reside in the sclera itself. When we work to find an appropriate vision correction for an eye that has a large primary ectasia, I believe it valuable to keep in mind that the sclera is to some degree an extension of the cornea. Some of the distortion seen in the cornea may also be found in the sclera.
While many clinics have no instrumentation for directly measuring “scleral astigmatism” or “scleral ectasia,” we can visualize it indirectly (see sidebar “A Case of Residual Astigmatism”). The scleral lens will sink into the conjunctiva while being worn. The longer it is worn, the deeper it will sink. As the lens gets larger and its haptic encroaches onto more sclera, it will begin to take on some of the toricity of the sclera, if it exists. When patients return for follow up complaining of poorer vision than when they received their lens, a sphero-cylindrical over-refraction is required. When the “unexpected” cylinder is revealed, use the corneal topographer to map the front surface of the “spherical” scleral lens in situ. If you find cylinder on the surface of the lens, the lens should be remade 0.1mm thicker. This 33% or so increase in center thickness stiffens the lens. It has less of a tendency to flex, and much of that cylinder should disappear.
While this tactic may help, it might not cure the problem. A fluid bath that simultaneously wets and protects the cornea and neutralizes the cornea’s irregularities refractively should allow the spherical scleral lens to provide a sharp and clear refraction. Unfortunately, this is not always the case. The best solution for vision in many cases is a pair of glasses to be used over the contact lenses to correct the residual cylinder and any minor spherical correction required.
Approaching Problems Involved with Mini-Scleral Lens Application
Mini-scleral lens application is very similar to that of corneal GP or soft contact lens application and involves proper hand preparation, lens preparation, eye opening, and lens application technique.
There are, however, three major differences between the placing of a scleral lens of any design on an eye and the placing of smaller lens designs: 1) the size of the lens, 2) that it must be centered over the cornea on application, and 3) that it must be filled to the brim with sterile, nonpreserved saline solution.
As is the case when applying any contact lens, hands must be clean, dry, and lint-free prior to scleral lens handling.
Patients should remove the lens from its soaking solution and fill the bowl with sterile, nonpreserved saline solution almost to overflowing. They must then balance the lens using two or three fingers, or on one finger using an orthodontic rubber band as a support; the lens may be placed on a lens holder that features suction-release capability (such as the DMV Classic [DMV Corporation]); or the lens may be rested on a stable base so both hands are free to fully open the eyelids to the extent that the lens will easily reach its on-eye destination (Figures 5 and 6).
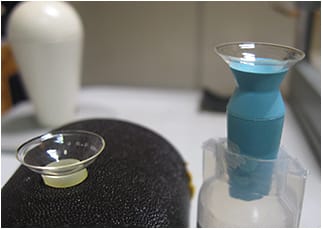
Figure 5. An orthodontic elastic and a stand for use with scleral lens application.
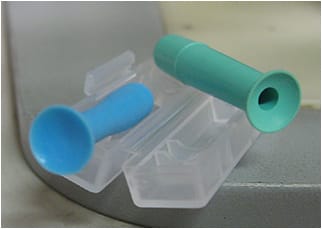
Figure 6. Two examples of scleral lens application/removal devices.
A Case of Residual Astigmatism
Our patient’s pre-contact lens refraction (2009) was LE: –5.25/–5.50 x 20, VA 6/12+ (20/40+). At this time the patient was fit with 10.2mm corneal keratoconus design GP contact lenses.
After three years, the patient returned wishing to be refit because of comfort issues. We offered a mini-scleral lens. Her response to the diagnostic lens was very encouraging.
Her pre-fitting topography image showed global keratoconus with central distortion and nearly 7.00D of sim-cylinder (Figure A).
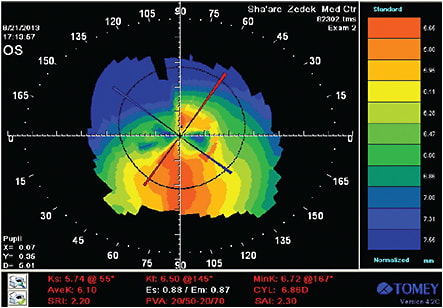
Figure A. Patient’s pre-contact lens topography map.
We ordered a lens in the following parameters: 4.60-S sagittal height, 15.8mm diameter, flat #1 edge, 0.3mm center thickness, –3.75D, VA 6/21 (20/70). Topography over the first scleral lens had the appearance of regular with-the-rule astigmatism of about 1.50D (Figure B). Over-refraction was plano/+1.75 x 85, VA 6/12.
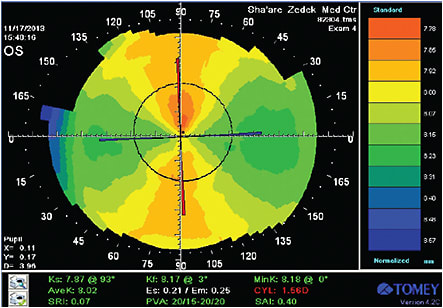
Figure B. Corneal topography over the first scleral diagnostic lens.
We reordered the lens in the following parameters: 4.70-S sagittal height, 15.8mm diameter, flat #1 edge with a toric haptic, 0.4mm center thickness, –3.00D. At the time of dispensing/exchanging the lenses, the patient was very happy with her improved vision, which was 6/12+ in the weaker eye.
At the two-week visit, we reviewed her over-refraction and topography. The topography showed an additional reduction in residual cylinder to 0.80D. Her manifest refraction was –0.50/+0.75 x 90 to a shaky 6/12. Figure C shows her topography over the final lenses. The patient is happy with her vision and comfort.
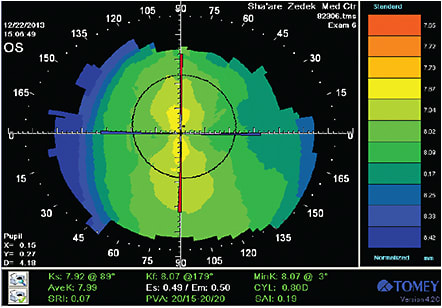
Figure C. Topography over the final lenses.
Bubbles The single most common problem with new scleral lens wearers is that of air bubbles, which primarily result from poor lens application technique. Either patients do not place enough saline into the bowl of the lens, or too much spills over as the eye enters the pool of fluid. A bubble can also form if the lens is manipulated and tilted while being worn, allowing air to enter under the edge of the lens and become trapped.
Bubbles under scleral lenses are obstructions to vision and potential irritants to the corneal epithelium. There are three signs of bubble existence about which you must educate patients and for which they must check on each lens application: 1) reduced vision, 2) reduced comfort, and 3) the appearance of large or small circular areas of different refraction of the iris and pupil when viewed with a mirror (Figure 7). If patients note these bubble signs, the lens must be removed, refilled with saline, and reapplied to the eye. A bubble that remains trapped will abrade and cause a red, painful, teary, and inflamed eye.
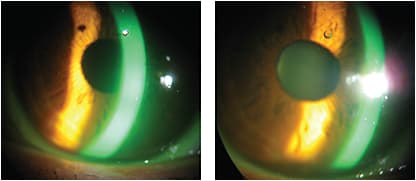
Figure 7. A small bubble highlighted in the band of fluorescein (left) and without fluorescein (right).
Removing Scleral Lenses
It is a fact that the haptic of a scleral lens sinks slowly and inexorably into the palpebral conjunctiva during lens wear. The longer the lens is on the eye, the deeper the lens settles. As the lens settles more and more, the attraction of the lens to the eye increases and the lens is more caught in the conjunctiva. Releasing a lens in this condition can be tricky and, if attempted incorrectly, painful.
The first step toward releasing a mini-scleral lens after a long wearing period is to apply a drop or two of an ocular wetting agent (anything from saline to more viscous artificial tear supplements). Second is the classic peri-haptic depression, which is intended to break the seal and import an air bubble under the lens. Patients should perform this both inferiorly and superiorly by pressing gently through the lids while gazing in the direction opposite to the lid depression. By this stage, either the lens will fall out when gently nudged at its edges with the lids, or it can be more aggressively released from the eye using a DMV lens remover (“Ultra”—no hole model, Figure 6). The recommended approach with the lens remover is to attach it to the lower third of the lens and remove in a sweeping upward arc motion, all the while holding the lids open.
Maximizing Wearing Time with Scleral Lenses
The object of many contact lens wearers is to maintain lens wear throughout all of their waking hours. Many do not reach this goal. The potential for scleral lens wearers to complete a long working day with their eyes still comfortable exists, but care must be taken to instruct wearers on how to reach this goal. Patients should be aware of the following: lenses must be kept clean; bubbles must not occur when applying the lenses; full blinking can help to control debris accumulation and improve surface wettability; and regular replenishment of the saline bath can revitalize the corneal surface.
A Worthy Effort
In a hospital-based specialty contact lens practice, our staff has had the privilege of being called upon to assist many patients who have problem corneae—and problem eyes. Many of those with whom I have worked and fit in mini-scleral lenses have done so well, they proclaim that they arise in the morning and thank me for my efforts.
On the other hand, I have learned much about the problems of fitting these lenses. One patient in particular who had very advanced keratoconus necessitated the order of 11 lenses for her left eye, and still the fit was incomplete. She has loose conjunctiva into which lenses would sink and the edges would be engulfed; the intracameral fluid would fill with debris; her eye would become red and uncomfortable. The patient is a laboratory technician in the hospital and cannot remove her contact lenses regularly for saline replacement. Even though this is a case with a prospectively poor outcome, these mini-scleral lenses have changed so many of our patients’ lives for the better that it continues to be worth a try. CLS
Acknowledgements
As always, my respect and thanks must be expressed to my patients for choosing me to help them confront their visual adversities invoked by their corneal ectasias.
I would be amiss if I did not include a kind word for my mini-scleral fitting mentors: the consultants at Blanchard Labs, Viscon Contact Lens, and Dr. Steve Byrnes.

|
Dr. Schendowich is a member of the Medical Advisory Board of the National Keratoconus Foundation, USA, a fellow of the International Association of Contact Lens Educators, and a clinical supervisor to Israeli optometry students in the ophthalmology clinic at the Sha’are Zedek Medical Center in Jerusalem, where he is a specialty contact lens fitter. |