


SCLERAL CASES
Scleral Lens Case Grand Rounds
These cases show how scleral lenses can greatly improve patients’ quality of life.
By Edward S. Bennett, OD, MSEd, FAAO; Gregory W. DeNaeyer, OD, FAAO; Melissa Barnett, OD, FAAO; Muriel Schornack, OD, FAAO; Stephanie Woo, OD, FAAO; & Derek J. Louie, MSc, OD, FAAO
Scleral lenses are the fastest growing GP option (see “GP Annual Report 2014” in this issue), primarily because of their ability to improve the quality of life of individuals who have corneal irregularity and severe dry eye. In many of these individuals, contact lenses had previously either not been indicated or could not provide adequate comfort, vision, or both. In particular, scleral lenses have been life changing for keratoconus patients facing surgery after failing with other lens options and for patients experiencing extreme discomfort from severe dry eye conditions.
As a result of their benefits of initial comfort (versus corneal GPs) and vision (versus soft lenses), scleral lenses are also finding increasing application for healthy eyes, notably astigmatic and presbyopic individuals.
This article presents representative cases in which scleral lenses greatly increased the quality of patients’ lives.
Case #1: Post-Keratoconus Corneal Graft, Part 1
History and Evaluation A 60-year-old female keratoconus patient presented to Dr. DeNaeyer’s practice for specialty lens evaluation. She had a history of bilateral penetrating keratoplasty and cataract surgery. A recent trauma to her right eye required her to have a second corneal graft and also left her aphakic. She developed secondary glaucoma in her right eye and, subsequently, underwent a trabeculectomy.
The patient’s entering visual acuity with her recent spectacles was OD +4.00 –4.00 x 072, Count Fingers at three feet and OS +2.00 –7.25 x 158, 20/50. She was initially interested in a contact lens for her left eye. Topography OS showed significant astigmatism and irregularity. Slit lamp examination revealed a clear graft without sutures (Figure 1).
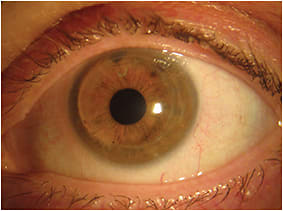
Figure 1. Post-penetrating keratoplasty in Case #1 showing a clear graft of the left eye.
Lens Fitting and Follow-up Care The patient’s left eye was diagnostically fit with a 16mm Europa (Visionary Optics) scleral contact lens with parameters of 52.00D base curve radius (BCR) and –6.00D power. The patient’s vision OS at the dispensing visit was 20/25. The scleral lens had complete central corneal clearance and fit without excessive compression (Figures 2, 3, and 4). (Click here to view a video of an optic section assessment showing acceptable clearance of a scleral lens courtesy of Dr. DeNaeyer.)
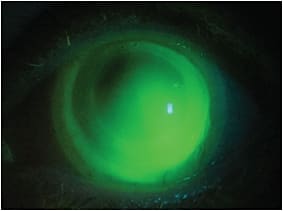
Figure 2. Scleral lens fluorescein pattern in the left eye in Case #1.
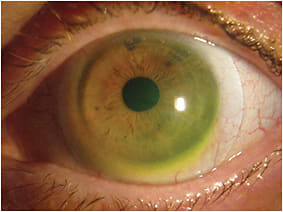
Figure 3. The left scleral lens in Case #1 shows centration and haptic alignment.
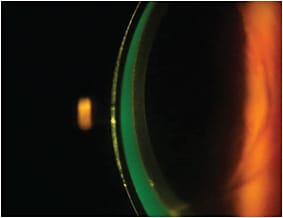
Figure 4. An optic section reveals good apical clearance for the left scleral lens in Case #1.
We prescribed a hydrogen peroxide care system for cleaning/disinfection and instructed her to fill the lens with 0.9% sodium chloride inhalation solution (off-label) pre-application. We also prescribed plano spectacles with a +2.50D add OD and OS over her contact lens for reading. She successfully wore the contact lens OS for four months and then decided that she would like to have the right eye fit as well.
The patient’s uncorrected visual acuity OD was 20/400 and did not improve with refraction. Topography showed significant astigmatism and irregularity. The right graft was clear with remaining buried, interrupted sutures, and the patient had traumatic mydriasis (Figure 5). An avascular conjunctival bleb was positioned just above the superior limbus, which was a significant factor when considering GP design options. It’s important that a GP lens not negatively affect the bulbar conjunctiva that forms the bleb because damage to this tissue could result in a bleb leak.
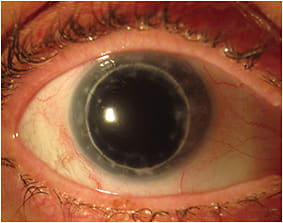
Figure 5. Corneal graft of the right eye in Case #1.
We diagnostically fit a mini-scleral lens that had a diameter of 15mm and a pre-cut notch to bypass the filtering bleb. The diagnostic lens had a 47.00D BCR and exhibited central corneal touch and peripheral edge lift (Figure 6). The notch appeared to be wide enough to accommodate the bleb. A notched, 15mm scleral lens was ordered with a 51.00D BCR and –2.25D power, which was determined from over-refraction of the diagnostic lens.
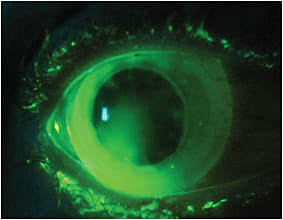
Figure 6. Initial diagnostic lens for the right eye in Case #1 demonstrating central corneal touch and peripheral edge lift.
At the dispensing visit, the patient’s visual acuity OD measured 20/30. The lens had adequate central corneal clearance, and the notch adequately bypassed the conjunctival bleb (Figure 7). The rest of the haptic section fit well without edge lift or compression. We instructed the patient to apply the lens with the notch at the 12 o’clock position.
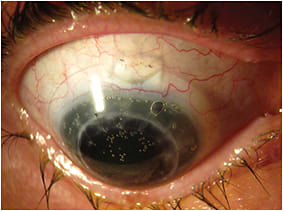
Figure 7. The final lens for the right eye in Case #1 showing the notch in the lens adequately bypassing the conjunctival bleb.
At a follow-up appointment, the patient reported doing “great” and was pleased with the vision and comfort that the lenses provided. No secondary contact lens complications were observed, and the conjunctival bleb OD remained healthy.
Discussion Patients who have undergone penetrating keratoplasty may need GP lenses postoperatively to correct regular or irregular astigmatism. Scleral contact lenses are often a good choice for patients who have moderate-to-severe irregularity, especially when combined with oblique or against-the-rule astigmatism. Make sure to obtain approval from the corneal surgeon before fitting a postoperative patient.
Choose materials that have hyper-oxygen permeability (Dk) to avoid corneal hypoxia. If a patient has symptomatic corneal swelling with lens wear, his endothelium may not be healthy enough to wear a scleral lens. In these cases, refit the patient into a smaller corneal GP. Ocular irritation and redness may not always be secondary to a poor fit, but rather may result from a corneal graft complication such as graft failure or secondary glaucoma. If you are fitting a corneal graft patient who has also undergone a filtering surgery, make sure the scleral lens is not causing injury to the conjunctival bleb. Having a notched diagnostic scleral lens on hand is helpful during the initial fitting. Photographing the lens can help the laboratory adjust the size of the notch to help minimize interaction between the scleral lens and the bleb. A relatively small-diameter lens reduces the required notch size, which decreases the likelihood of the notch inducing bubbles. Instruct patients to always line the notch up with the bleb during lens application.
Case #2: Post-Keratoconus Corneal Graft, Part 2
History and Evaluation A 52-year-old Caucasian female presented to Dr. Schornack’s practice for possible scleral lens wear in February 2012. The patient had been diagnosed with keratoconus as a teenager, and she had undergone penetrating keratoplasty in the left eye in 1991. She had worn corneal GP lenses since her diagnosis with reasonable success. However, during the two years immediately prior to her presentation for scleral lens evaluation, she experienced increasing discomfort with both corneal lenses. One year prior to her examination, she developed a corneal dellen just peripheral to the graft-host junction in the infero-nasal quadrant in the left eye, which resulted in thinning of the host tissue. At the same time, progression of keratoconus in the right eye was causing increasing lens intolerance. Attempts to refit the corneal GP lenses in a piggyback system and to fit hybrid lenses failed.
At the time of presentation for scleral lens evaluation, the patient was able to tolerate her corneal GP lenses for approximately three to four hours daily in her right eye and six hours daily in her left eye. To maintain functional vision for most of the day, she wore only one lens at a time. In general, she wore her right lens in the morning and then switched to her left lens for the afternoon and evening hours. She was also considering additional surgical intervention (lamellar keratoplasty for the right eye and repeat penetrating keratoplasty for the left eye).
Her visual acuity with her corneal GPs was 20/40 OD, 20/20- OS. Figure 8 shows her axial topographic images. Slit lamp evaluation revealed no significant corneal opacity in the right eye, but the apex of the cone was obvious with an optic section (Figure 9).
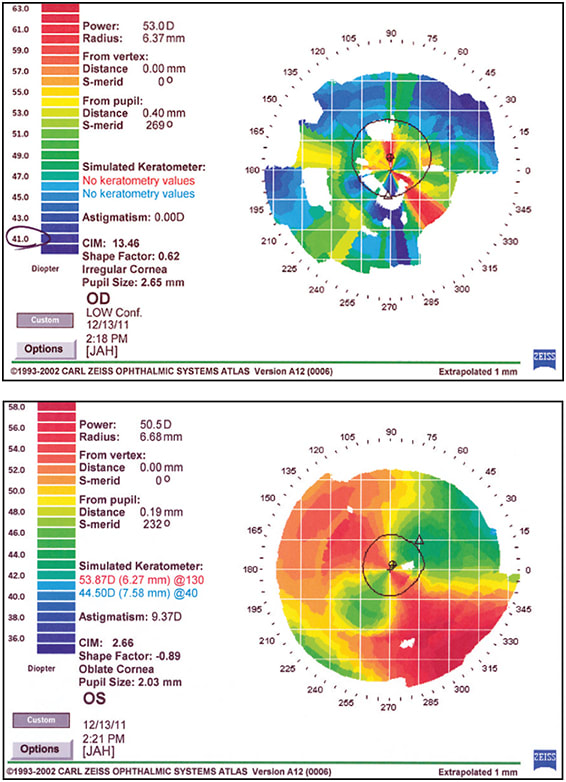
Figure 8. Corneal topographic images of the patient in Case #2, with the top showing the right eye and the bottom showing the left eye.
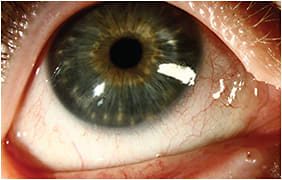
Figure 9a. Diffuse slit lamp image revealing no corneal opacification of the right eye in Case #2.

Figure 9b. The thinning of the corneal apex as shown with optic section of the right eye in Case #2.
In the left eye, the graft was clear, but thinning of the host tissue in the infero-nasal quadrant was clearly visible on slit lamp evaluation (Figure 10) and Scheimpflug imaging (Figure 11).
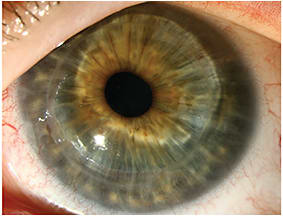
Figure 10. Slit lamp evaluation showing a clear corneal graft and thinning of the host tissue in Case #2.
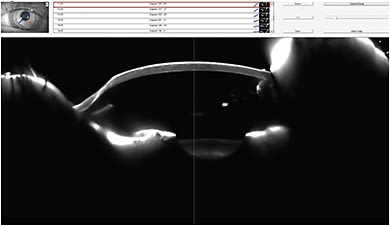
Figure 11. Scheimpflug image showing thinning of the host tissue in the inferior-nasal quadrant of the left eye in Case #2.
Lens Fitting and Follow-up Care We ordered a standard Jupiter (Essilor, Visionary Optics) 18.2mm overall diameter (OAD) lens for the right eye. This lens exhibited a good fitting relationship, but provided only 20/40 acuity. Sphero-cylindrical over-refraction resulted in 20/25 acuity, so a front-surface toric lens was ordered. With this lens, the patient was capable of 20/20-2 OD. Figure 12 shows the position of the toric indicators on the anterior surface of the lens prescribed.
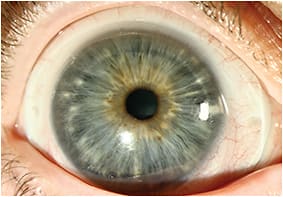
Figure 12. Scleral lens for the right eye of Case #2 showing the position of the toric indicators on the anterior lens surface of this front-surface toric design.
For the left eye, Figure 11 shows that the entire graft is elevated and rather flat. We fit a custom Jupiter lens that provided a larger optical zone and steeper inner peripheral curve radius (PC 1) compared to the standard Jupiter design. Lens settling after several hours of wear completely eliminated lens clearance at the graft-host junction, and the lens decentered temporally. This resulted from the relatively short distance in the patient’s left eye between the nasal limbus and the caruncle.
The second lens ordered featured a steeper PC 1 and slightly reduced PC 3 and PC 4 widths to avoid contact with the caruncle (to improve centration). The second lens completely cleared the cornea (Figure 13) and provided 20/20 acuity.
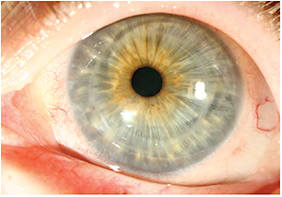
Figure 13. Slit lamp evaluation of the final scleral lens prescribed for the left eye in Case #2.
The final lens parameters OD were:
• BCR/OAD/optical zone diameter (OZD): 6.75mm/18.2mm/8.2mm
• PC 1 radius/width (R/W): 7.15mm/2.0mm
• PC 2 R/W: 9.0mm/1.0mm
• PC 3 R/W: 12.25mm/1.5mm
• PC 4 R/W: 14.5mm/0.5mm
• Prescription (Rx): –6.25 –2.50 x 175, Jupiter B, visual acuity (with lens) of 20/20
The final lens parameters OS were:
• BCR/OAD/OZD: 6.49mm/18.2mm/8.6mm
• PC 1 R/W: 6.60mm/1.8mm
• PC 2 R/W: 8.85mm/1.0mm
• PC 3 R/W: 12.25mm/1.3mm
• PC 4 R/W: 14.0mm/0.4mm
• Rx: –13.25D, Jupiter custom, visual acuity (with lens) of 20/20
The patient returned for a follow-up visit 18 months later. She noted no change in vision or comfort, but the visual acuity in the right eye had decreased to 20/50, and the left lens was now being entirely supported by the graft. Over-refraction OD indicated that the patient needed additional cylinder correction in the lens.
New lens parameters OD were:
• BCR/OAD/OZD: 6.75mm/18.2mm/8.2mm
• PC 1 R/W: 7.15mm/2.0mm
• PC 2 R/W: 9.0mm/1.0mm
• PC 3 R/W: 12.25mm/1.5mm
• PC 4 R/W: 14.5mm/0.5mm
• Rx: –6.50 –4.50 x 157, Jupiter B, visual acuity (with lens) of 20/25+1
New lens parameters OS were:
• BCR/OAD/OZD: 6.03mm/18.2mm/8.6mm
• PC 1 R/W: 6.48mm/1.8mm
• PC 2 R/W: 8.85mm/1.0mm
• PC 3 R/W: 12.25mm/1.3mm
• PC 4 R/W: 14.0mm/0.4mm
• Rx: –13.25D, Jupiter custom, visual acuity (with lens) of 20/20
The new lenses resulted in an acceptable fitting relationship and good vision.
Discussion There are several clinical pearls to be gained from this case:
1) Front-toric scleral lenses are stable and can do a wonderful job of correcting residual astigmatic refractive error.
2) You may wonder why the patient developed so much more cylinder in the right eye. This could potentially be due to progression of her disease, or it could simply have been because the corneal GP was removed. Remember that keratoconus affects the entire cornea, not just the anterior surface. We don’t exactly know how wearing a corneal GP lens changes deeper layers of the cornea, but it’s possible that some compression may have been occurring beneath the corneal lens. When the mechanical flattening force was removed, corneal contour (anterior, posterior, or stromal) may have changed.
3) Benefits of the scleral lens for the left eye included continuous hydration of the entire ocular surface. It is unlikely that a dellen will develop beneath a scleral lens.
4) I think of scleral lenses in cases like this as “bridges”; we may not be able to completely avoid surgery, but can certainly delay more aggressive intervention. If we can “buy” the patient just a few more years before a graft (or regraft), we allow time for surgical techniques to improve, and could potentially decrease the total number of grafts and regrafts necessary during a patient’s lifetime.
Case 3: Post-Refractive Surgery, Part 1
History and Evaluation A 38-year-old male presented to Dr. Louie’s clinic in June 2014 with a left eye that had been red for the past three weeks, with mild mucus, light sensitivity, and tearing. He was able to tolerate his contact lens for only one hour before it became unbearably painful. Lens removal completely alleviated the symptoms. He reported that his vision was somewhat blurry, but he was not sure whether it was better or worse than previously without correction. His uncorrected vision (left eye) was 20/300 at the time of examination. He did not wear a contact lens on the right eye, which had uncorrected vision of 20/20 and was problem-free. He reported wearing the same left lens prescribed since the last visit.
The history included a previous, uncomplicated LASIK surgery in both eyes in 2009. In 2011, the patient was diagnosed with post-LASIK ectasia OS only. As no pre-operative data was available, we are unable to ascertain whether this was a case of forme fruste keratoconus before the refractive surgery. His past ocular history was unremarkable for other eye conditions. He denied any previous injury or significant ocular or systemic disease in either eye. His last dilated fundus examination was in 2011.
The patient was previously fit in 2012 with a Duette (SynergEyes) hybrid lens (left eye only) in parameters of 7.1mm BCR, 14.5mm OAD/steep skirt, –7.50D power with best contact lens-corrected visual acuity of 20/40. At that time, the contact lens assessment was “thin visible fluorescein layer under GP portion of lens, thinner superior versus inferior, moves 0.5mm with blink, bearing in soft skirt landing zone, slight infero-temporal decentration, good comfort.” The prescription was released at that time, and the patient was asked to return in one year.
It was assumed, but not verified by lens assessment, that the hybrid lens was now fitting flat, with significant apical touch that caused apical staining and possibly corneal abrasion, leading to the patient’s symptoms of irritation, tearing, photophobia, and pain. Additionally, the lens had passed its recommended replacement schedule, and there were likely components of contact lens overwear and/or contact lens-associated red eye. Table 1 presents the patient’s anterior segment evaluation.
| RIGHT EYE | LEFT EYE | |
|---|---|---|
| Adnexa | Normal | Normal |
| Lids/Lashes | Normal | Normal |
| Conjunctiva/Sclera | White and quiet | White and quiet |
| Cornea | Central iron deposit in anterior stroma; LASIK scar on peripheral cornea; flat, intact LASIK flap | 2 to 3+ staining at inferior apex, LASIK scar on peripheral cornea; flat, intact LASIK flap |
| Anterior chamber | Deep and quiet | Deep and quiet |
| Iris | Round and reactive | Round and reactive |
| Vitreous | Clear | Clear |
We instructed the patient to discontinue his habitual lens and initiate Pred Forte (prednisolone acetate, Allergan), 1 gt q.i.d. for two weeks OS. The plan was to refit the left eye with a scleral lens that vaults the entire cornea if the current symptoms were resolved at the two-week corneal evaluation.
Lens Fitting and Follow-Up Care At the two-week follow-up visit, the patient reported resolution of all previous symptoms, except persistent blur OS. Pentacam (Oculus) corneal topography was performed to assess corneal thickness and curvatures for future monitoring of ectasia (Figures 14 and 15).
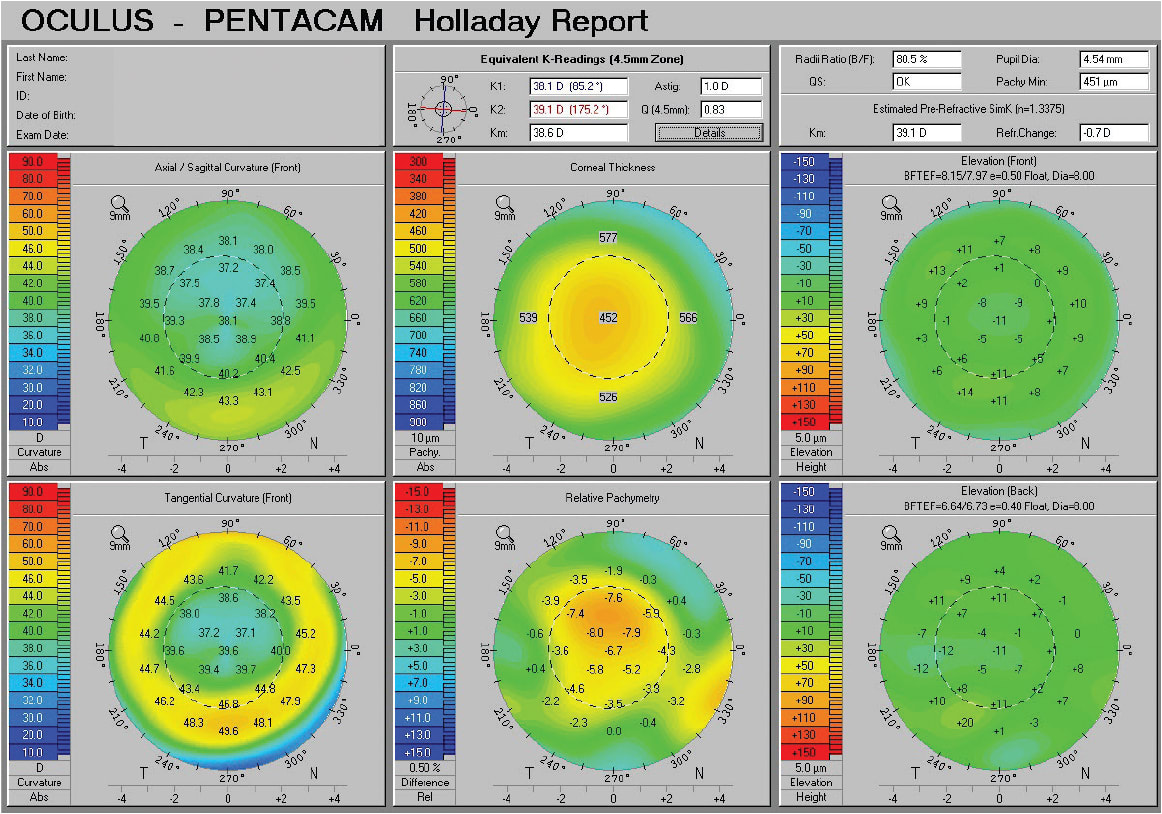
Figure 14. Corneal topography of the left eye in Case #3.
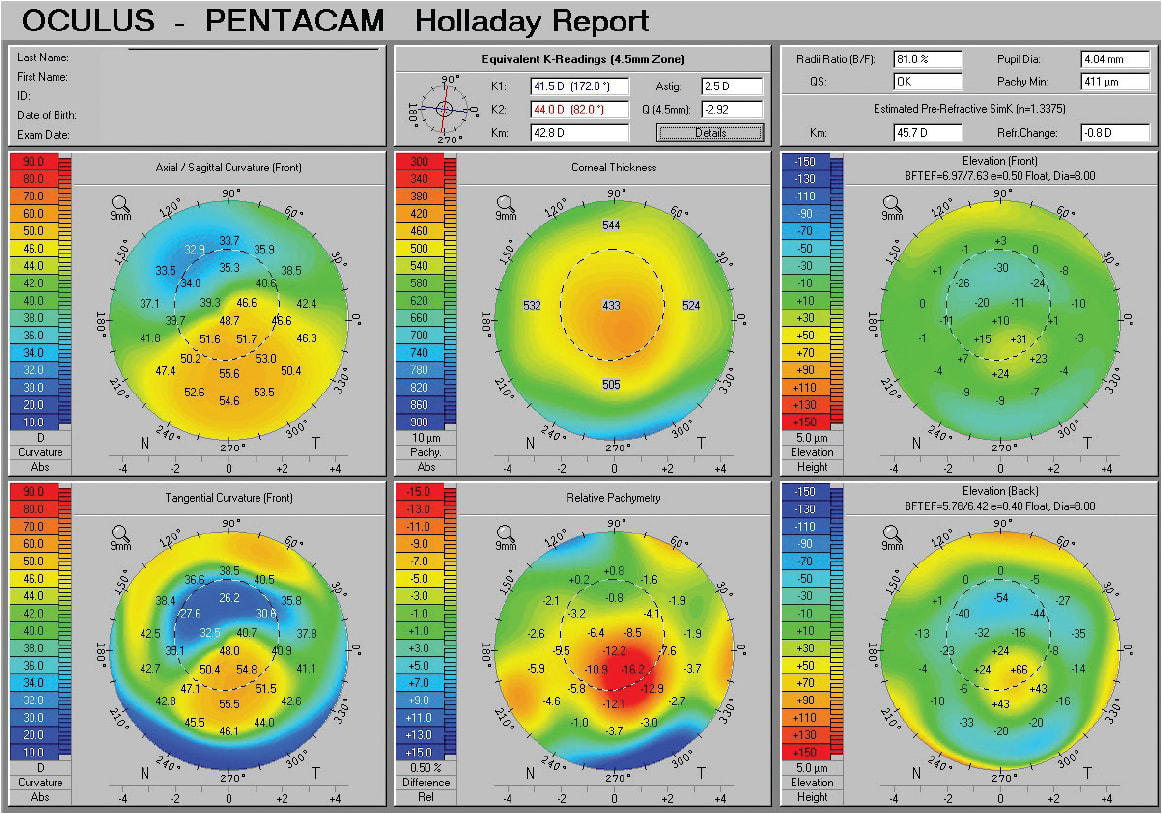
Figure 15. Corneal topography of the right eye in Case #3.
We refit the patient successfully, left eye only, with a Custom Stable (Valley Contax) scleral lens in parameters of 8.23mm BCR, 15.8mm OAD, plano power, standard limbal curve, 1 flat scleral landing curve in the Boston XO (Bausch + Lomb) material. The Custom Stable scleral lens design incorporates a standard reverse geometry peripheral curve system to enhance corneal vault and help minimize limbal bearing with lens settling. Custom Stable lenses also include digital radial edge profiles to minimize lid interaction and conjunctival impingement. The lens had 300 microns of clearance over the apex of the cornea, clearance over the limbus for 360º, a slight inferior decentration, and good apposition to the sclera, with no apparent vessel blanching or conjunctival impingement at the most recent assessment after four hours of wear. The patient reported comfortable wear during waking hours, with stable 20/25 vision OS (Figure 16). The limitation on achieving crisp 20/20 acuity is likely due to the remaining posterior corneal irregularity (posterior float/curvatures OS seen in Figure 14), as no other ocular pathology was identified during this examination.
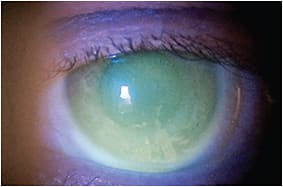
Figure 16. The left eye scleral lens-to-cornea fitting relationship in Case #3.
Discussion A reverse geometry scleral lens design, similar to a reverse geometry corneal lens, can enhance corneal clearance without requiring an excessively steep central base curve to vault corneal irregularity in the traditional flatter (than BCR) peripheral curve radius designs. A flatter central BCR also decreases the need for higher myopic correction to compensate for steep curve radii, which leads to a more consistent lens thickness and presumably to more consistent oxygen transmission (Dk/t). With reverse geometry scleral lens designs, practitioners must be cognizant of the limbal zone. Excessive reverse curves and smaller chamber size can result in the lens resting on, or anterior to, the limbus; this could cause limbal flush, an indication of excessive interaction of the lens with the limbal stem cells. A small amount of limbal vault (i.e., less than at the central cornea) is always necessary and should be monitored by observing the limbus for injection and staining immediately after scleral lens removal.
Case 4: Post-Refractive Surgery, Part 2
History and Evaluation A 55-year-old female entered Dr. Bennett’s clinic for a contact lens fitting for her left eye in January 2012. She complained of blurred vision, which made driving very difficult, and chronic dry eyes. She was interested in whether a contact lens may improve her vision. She underwent bilateral 16-incision radial keratotomy in 1990 (Figure 17). She ultimately had a retinal detachment OD with a resulting vitrectomy, and the ensuing complications resulted in hand-motion vision. Therefore, she was wearing spectacles with a balance lens OD and visual acuity of 20/30- (with difficulty) OS. She also had grade 1+ nuclear sclerosis OS.
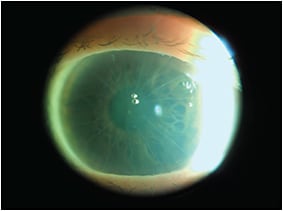
Figure 17. Initial corneal presentation of radial keratotomy in Case #4.
Lens Fitting and Follow-up Care With corneal topography, her sim Ks OS were 39.4 @ 086/38.9 @ 176. We initially fit an 11.2mm diameter intralimbal lens design, but it exhibited excessive movement and decentered inferiorly.
We then fit a Jupiter scleral lens from Essilor in parameters of 8.3mm BCR, 16.0mm OAD, –5.75D power. Greater than 200 microns of clearance was noted after initial settling, and there was no sign of blanching. With a plano over-refraction, the patient was correctable to 20/20. We ordered lenses in parameters of 8.23mm BCR, 15.6mm OAD, reverse geometry, and –5.75D power. The patient was also provided with Refresh Liquigel (Allergan) OD and preservative-free lubricating drops OS for her dry eyes, and she was educated about optimizing her environment (e.g., the need to blink more when performing computer work and keeping vents from blowing air directly on her eyes).
The lens at dispensing exhibited an optimum fitting relationship with evident tear exchange, 200 microns of central clearance, and no peripheral seal-off or blanching. Her visual acuity was 20/25-. She was quite pleased with the vision and comfort at the one-week visit, and the fitting relationship still looked quite good. She was wearing the lenses for 12 hours per day.
At the one-month follow-up visit, the patient indicated that she was experiencing mild lens awareness. Slit lamp evaluation revealed localized areas of nasal and temporal conjunctival blanching of vessels. We then ordered the lens with a slightly flatter periphery (i.e., third curve 1mm flatter; fourth curve 0.5mm flatter per laboratory consultant). This lens did not completely resolve the problem. Upon consultation, we ordered a new lens with a larger OAD and flatter peripheral curve radius in the following parameters: 8.23mm BCR, 16.4mm OAD, –5.75D power.
Upon dispensing, this lens provided 20/25 visual acuity with adequate central clearance (200 microns after 15 minutes, Figure 18), good limbal clearance, and edge alignment. In two follow-up visits (at two weeks and three months later), she reported good vision, which allowed her to drive, and good comfort. Her wearing time was 12 hours a day, and she was very satisfied.
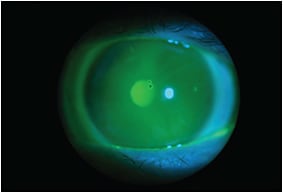
Figure 18. Final scleral lens-to-cornea fitting relationship for left eye in Case #4.
Discussion This is a good example of how valuable laboratory consultants are in guiding clinicians toward a successful fit. Both a “Contact Lens Consultants FAQ” module and numerous webinars on scleral lenses are available at www.gpli.info.
Case 5: Ocular Surface Disease
History and Evaluation A 58-year-old Caucasian female presented to Dr. Barnett’s practice with a history of dry eyes, particularly status post-blepharoplasty for the upper and lower eyelids of both eyes. She complained of red, burning, tearing, and photophobic eyes since her surgery. Ocular history was also significant for a posterior subcapsular cataract in the right eye. She previously wore soft contact lenses (both daily disposable and two-week replacement lenses). Ocular medications included topical cyclosporine 0.05% one to two times a day and artificial tears one to two times a day. However, there was no improvement with the eye drops.
Her medical history was significant for recurrent Herpes simplex virus. Medications taken were estradiol, progesterone, and Valtrex (valacyclovir hydrochloride, GlaxoSmithKline).
Visual acuity with spectacles was 20/25+1 in the right eye (improved to 20/20+1 with pinhole) and 20/40-2 in the left eye (improved to 20/25+1 with pinhole). Manifest refraction of –10.25 +1.00 x 160 in the right eye enabled 20/20-2. Manifest refraction of –8.50 +0.75 x 091 in the left eye enabled 20/20-2.
Sim-K readings with topography were OD 42.35 @ 065/42.24 @ 155 and OS 42.72 @ 098/41.82 @ 008. There was irregular astigmatism in the right eye and regular astigmatism in the left eye.
Slit lamp examination revealed 1+ meibomian gland dysfunction in both eyes. Conjunctival staining (2+) and chemosis (1+) were present in both eyes, and both eyes had a reduced tear meniscus. Corneal staining was visible in both eyes, the right eye worse than the left. Tear breakup time was two seconds in the right eye and four seconds in the left eye. Both eyes had normal intraocular pressures. Trace nuclear sclerosis was present in both eyes. The right eye had a posterior subcapsular cataract. Optic nerves and maculae were normal in both eyes.
Lens Fitting and Follow-up Care We fit scleral lenses with a 16.5mm diameter in both eyes. Lens parameters were OD 41.00D BCR, 16.5mm OAD, 9.5mm OZD, sag 4.63, –8.00D power and OS 41.00D BCR, 16.5mm OAD, 9.5mm OZD, sag 4.63, –6.50D power. Visual acuity in each eye was 20/20-1. The right eye had an over-refraction of +0.25D. No over-refraction was present in the left eye. Binocular vision without an over-refraction was 20/15.
Both lenses exhibited good central apical clearance. There was less clearance superior nasal; however, the lens cleared the cornea in each eye. The lenses fit well peripherally without blanching (Figure 20). There was no evidence of sebaceous tear debris nor surface debris on either lens.

Figure 20. Slit lamp evaluation of the scleral lens on the right eye in Case #5.
The patient reported “tremendous improvement” with her symptoms of ocular dryness. She did not experience dry eye symptoms and did not need artificial tears while wearing scleral lenses, and she was happy with the vision and comfort. However, without the lenses, the patient continued using nonpreserved artificial tears and cyclosporine 0.05% twice a day.
Discussion The benefits provided by full scleral lenses to dry eye patients have been known for many years. The increasing availability of different mini-scleral lens designs has resulted in a great increase in scleral lens use and a resulting increase in patient quality of life. This represents a very important application of these designs.
Case 6: Presbyopia
History and Evaluation A 61-year-old African-American male presented to Dr. Woo’s clinic for a comprehensive eye examination and contact lens evaluation in March 2014. He had been wearing corneal GP multifocals of unknown parameters for 10 years. The current pair was about two years old. He had no significant health or ocular history. His distance visual acuity with his current GP lenses was 20/30 OD, 20/50 OS, and 20/30 OU. His near visual acuity was 20/30 OD, 20/40 OS, and 20/30 OU. A sphero-cylindrical over-refraction over the habitual contact lenses resulted in no significant findings or improvement in vision in either eye.
The lens-to-cornea fitting relationship showed lid attachment OD and OS, with good centration and average edge lift. Both lenses were slightly scratched and had mild deposition.
With the lenses removed, the corneas had a very small amount of punctate staining in each eye near the inferior periphery. Other ocular health findings were unremarkable except for 1+ nuclear sclerotic cataracts in each eye. Posterior fundus photographs were unremarkable.
Keratometry values were OD 45.25 x 45.50 @ 095 and OS 44.25 x 45.25 @ 088. Mires were distinct and clear. Subjective refraction yielded OD –7.75 +0.75 x 096, 20/20 and OS –6.25 +0.75 x 081, 20/20. His near vision was 20/20 OD, OS, and OU with a +2.50D add.
We then discussed contact lens options. The first was to continue with corneal GP multifocals. An aspheric near design seemed most appropriate for this patient. Scleral multifocal lenses were also discussed. The patient was interested in trying to improve both his distance and near vision. He was also interested in decreasing the dryness that he experienced with corneal GP lenses. He was further intrigued with the idea of reducing lens dislodgement. After a comprehensive discussion of different lens options, we decided to proceed with scleral contact lenses.
Lens Fitting and Follow-up Care The patient returned for a scleral lens fitting in April 2014. We first determined eye dominance using two different tests, which both confirmed that the patient was right-eye dominant. I diagnostically fit Blanchard OneFit P+A Multifocal lenses in Boston XO in parameters of OD 7.10mm BCR, 14.6mm OAD, –6.25D power and OS 7.20mm BCR, 14.6mm OAD, –5.00D power. Upon application, each lens showed about 280 microns of clearance. After settling, the OD central clearance was 213 microns (Figure 21), and the OS central clearance was 216 microns (Figure 22). With sphero-cylindrical over-refraction, the patient attained 20/20 vision in each eye.
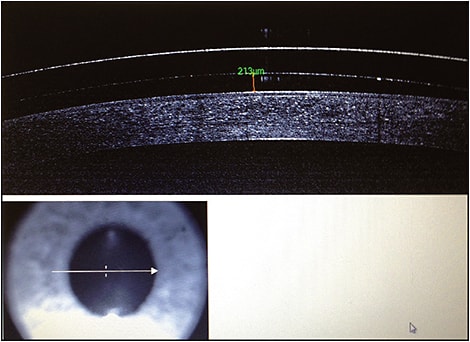
Figure 21. OCT image of the right scleral lens for the patient in Case #6.
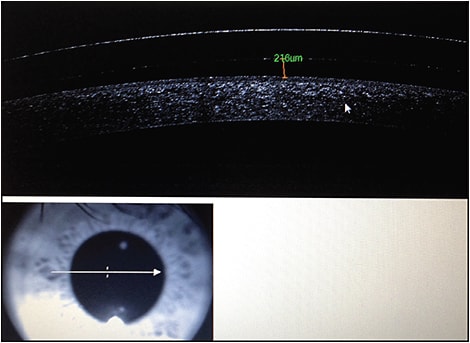
Figure 22. OCT image of the left scleral lens for the patient in Case #6.
We ordered Blanchard Onefit P+A Multifocal lenses in Boston XO in parameters of OD 7.10mm BCR, 14.6mm OAD, –9.75D power, dominant/dot and OS 7.20mm BCR, 14.6mm OAD, –9.00D power, nondominant. Table 2 presents the vision and fit assessment findings after the lenses had settled for about 20 minutes. The patient reported great comfort and was thrilled with the vision.
| OD | OS | OU | |
|---|---|---|---|
| Distance VA | 20/25 | 20/25 | 20/20 |
| Near VA | 20/30 | 20/30 | 20/25 |
| Central clearance | 210µm | 188µm | |
| Limbal fit | Full clearance about 50µm | Full clearance about 50µm | |
| Edges | Aligned, no blanching | Aligned, no blanching |
The patient returned for one-week and one-month follow-up visits. He was still very satisfied with the lenses and claimed, “This is the best vision of my life.” His corneal health was excellent with no staining or edema. The vision remained 20/20 at distance and 20/20 at near binocularly.
Discussion Some of the most exciting advances in scleral lenses are their applications for normal corneas. Several companies have developed scleral lenses for normal eyes. Relatively small diameters of 14.3mm to 14.9mm are familiar to current soft lens wearers, so patients are less apprehensive to try them. The oxygen permeability (Dk) of scleral lenses is very high and can help reduce/eliminate neovascularization observed in some contact lens patients. Good patient candidates include the following:
1) High plus or minus soft lens wearers
2) High astigmats
3) Patients experiencing dry eye with their current contact lenses
4) Current GP patients complaining of lens dislodgment, discomfort, or irritation
5) Presbyopes
6) All normal corneas
If your soft or GP lens patients desire crisp vision and great comfort with their lenses, consider scleral lenses as an option.
Making Our Case for Scleral Lens Fitting
These cases represent only a few of the large (and increasing) number of patients whose quality of life was made significantly better by scleral lens designs. With newer designs and the ability to customize the posterior surface to better fit highly irregular corneas, the future looks even brighter. CLS
|
Dr. Bennett is assistant dean for Student Services and Alumni Relations at the University of Missouri-St. Louis College of Optometry and is executive director of the GP Lens Institute. You can reach him at ebennett@umsl.edu. |
|
|
Dr. DeNaeyer is the clinical director for Arena Eye Surgeons in Columbus, Ohio, and a consultant to Visionary Optics, B+L, and Aciont. He has financial interest in the Europa (Visionary Optics) scleral lens. You can contact him at gdenaeyer@arenaeyesurgeons.com. |
|
|
Dr. Barnett is a principal optometrist at the UC Davis Medical Center in Sacramento, Calif. She is an advisor to Acculens, Alcon, and Allergan, has received honoraria from Alden Optical, and has performed research for Nidek. Dr. Barnett serves as secretary of the Scleral Lens Education Society. |
|
|
Dr. Schornack is a consultant in the department of ophthalmology at the Mayo Clinic in Rochester, Minn. She holds the rank of assistant professor in the Mayo Medical School. She is a founding member of the Scleral Lens Education Society and serves on the organization’s board of directors. |
|
|
Dr. Woo currently practices at Havasu Eye Center in Lake Havasu, Ariz. She is also the public education chair for the Scleral Lens Education Society and is an Advisory Board member for the GPLI. She is a consultant to Blanchard, X-Cel, and SpecialEyes. |
|
|
Dr. Louie is a clinical associate professor of ophthalmology at the Oregon Health & Science University. He is also the director of the Contact Lens Fellowship program at the Casey Eye Institute. He has received travel expenses from Valley Contax. |