


HYBRID LENSES
Troubleshooting Hybrid Lenses
Knowing how to overcome issues will improve your success with hybrid contact lenses.
By Jeffrey Sonsino, OD, FAAO
Hybrid lenses, which have been around since the 1980s, are not quite GP lenses and not quite soft lenses. The question is: So how do they behave? The answer: They don’t behave like either.
Those who understand the technology have had excellent success with hybrids, but this success did not occur overnight. When you practice at the forefront of contact lenses, a learning curve is associated with even the simplest new technology. To that end, learning troubleshooting techniques is the building block required for mastery. Once you grasp those techniques, the rest will come with your clinical experience, time, and patience.
If you are looking for lenses that can be applied with little skill and understanding, then hybrids are probably not for you or your patients. But, if you desire to learn how to fit lenses that can offer superior comfort, optics, and centration, you will be rewarded with the most loyal patients in the industry.
Traditionally, hybrid lenses have a large-diameter GP central zone surrounded by a peripheral zone made of soft material. Material and design changes alone have contributed to solving some past issues. The soft skirt of the latest hybrid designs is now a silicone hydrogel (SiHy) material with an oxygen permeability value (Dk) of 84. That is far greater than the HEMA skirt Dk of 9.3. This can eliminate or minimize neovascularization and other hypoxic effects that sometimes occur with the previous-generation hybrids (Pilskalns et al, 2007; Papas, 2006).
Also, being a SiHy material means that the skirt doesn’t bind (Brennan and Bruce, 1995; Swarbrick and Holden, 1994; Dumbleton and Jones, 2008). This is true of most SiHy materials in general. During the polymerization process, the silicone molecules “migrate” to the surface, thus trapping the water inside of the contact lens, like a sandwich. Silicone is hydrophobic, repelling the water molecules and keeping them inside the lens. This creates a situation with less tightening of the lens and significantly less lens binding.
Second-generation hybrids have key advantages and design changes over previous generations. For UltraHealth hybrid contact lenses (SynergEyes), the previous inner landing zone has been broadened and the soft skirt has been redesigned to include a thickened outer landing zone (Figure 1). This new design creates an enhanced tear pump, ensuring a continuous exchange of fresh tears throughout the day. We know this because casual observers can discern the rapid disappearance of sodium fluorescein instilled within the bowl of the lens when applied onto the eye.
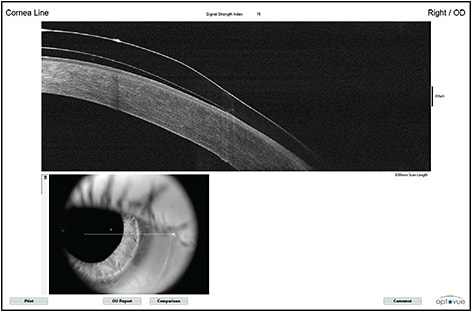
Figure 1a. Use of optical coherence tomography (OCT) to show the junction profile of an older-generation Synergeyes KC lens on a keratoconic eye. Note the basic design of the transition between the GP and hydrogel soft lens portions.
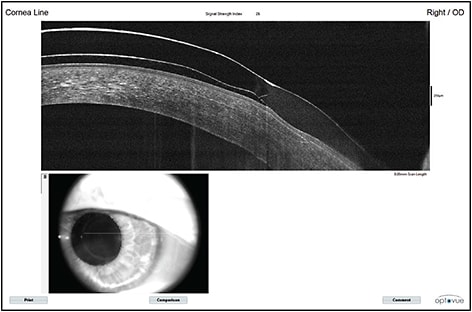
Figure 1b. Junction profile of the newest-generation UltraHealth lens on a keratoconic eye. Note the reverse geometry inner landing zone transitioning to a broader, cushioning SiHy soft skirt.
The combination of new SiHy materials, the newly designed inner and outer landing zones, and the updated philosophy of fitting the skirts flatter also has substantially reduced the tight lens issues experienced with the previous-generation hybrid lenses. The troubleshooting techniques here will focus on only the newest-generation materials. There are two classes of hybrid lenses: those for normal corneas and those for irregular corneas. Troubleshooting each class has its own nuances.
Hybrid Designs for Normal Corneas
The Duette HD and Duette Progressive (SynergEyes) are now recommended to be fit empirically using a base curve radius equal to the flatter keratometry reading (i.e., “on K”). This offers all of the advantages of fitting a GP lens on alignment, better vision, less flexure, and better comfort, but the soft SiHy skirt helps prevent decentration (Figure 2). With empirical fitting, you may face a number of issues.
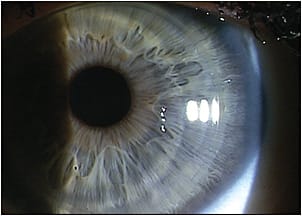
Figure 2a. Anterior segment photography of a well-fit Duette HD lens on a normal cornea. Note the proper centration denoted by the position of the junction.
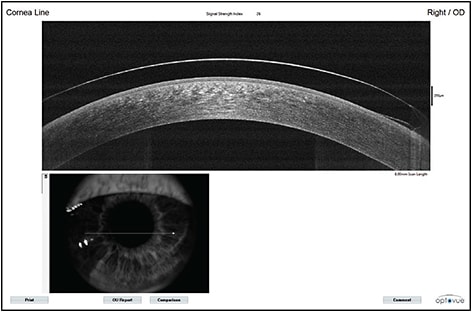
Figure 2b. Anterior segment OCT of a well-fit Duette HD lens on a normal cornea. The lens is fit “on K,” so an alignment fitting is expected, with edge lift at the junction between GP and soft SiHy skirt.
Lens Power More times than not, there will be a small over-refraction at the first dispensing appointment of the empirically designed lenses. This is anticipated. Practitioners should set patient expectations to realize that the first lens may not be the final lens.
Keep in mind that your over-refraction after dispensing should be approximately ±0.50D. If it is outside of that range, re-check the keratometry and refraction. If you find a cylindrical over-refraction, then there is residual astigmatism; these lenses do not perform well with residual astigmatism greater than about 1.00D (similar to a spherical GP when the patient has significantly more spectacle astigmatism than corneal astigmatism). Routinely auto-refract over lenses at follow-up visits to save time and tell whether there is a cylinder component to the over-refraction.
Comfort With hybrid lenses, patient comfort will be far better than with corneal GP lenses right from the start. If patients are habitual soft lens wearers and experience lens awareness, instruct them that this will pass after two days of lens wear. However, a steep skirt is one of the main reasons for true discomfort (not just lens awareness). If this is the case, and the patient has a difficult time removing the lenses, then flatten the skirt curve. Generally, reordered skirt curves go in the flatter direction. There are a few instances, however, for which a skirt curve must go steeper. One of these is when the skirt is fluting at the edge. Edge fluting will also cause lens awareness.
Another reason to steepen the skirt curve is when a Duette Progressive lens decenters. Proper functioning of the center-near multifocal is dependent on a centered lens. If there is temporal decentration (the most common direction of decentration), then steepen the skirt by one step. Temporal decentration of the center-near optics is almost always responsible for complaints of decreased vision at distance and near. This is evident at the dispensing appointment and is visible on white light biomicroscopic evaluation.
Occasionally, patients will have a comfort complaint due to the skirt folding in on itself (Figure 3). When removed, it will appear as a crease in the skirt. To remedy this, simply rehydrate the lens in a contact lens storage case for five to 10 minutes. The crease will disappear, and the lens can be reapplied.
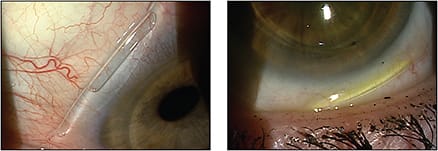
Figure 3. Two examples of skirts folded in on themselves. This is most likely a result of operator error during lens application. The lens must be removed and rehydrated in multipurpose contact lens solution.
The technique for applying the Duette HD and Duette Progressive lenses is similar to a soft lens. However, to assure that there are no application bubbles, one drop of artificial tears is instilled in the lens prior to application. We have found that it is not necessary to use a nonpreserved artificial tear solution due to the rapid tear exchange under the lenses.
Bubbles under a hybrid lens (Figure 4) usually result from poor application technique. Even a small application bubble at the junction (the most common site) will nearly always result in poor initial comfort. If left alone, comfort problems will result over time. The best way to avoid this simple problem is to ensure that the patient is using the artificial tear upon application.

Figure 4. Anterior segment photography of multiple application bubbles. This does not represent a fit that is too steep, as the UltraHealth lens is designed to vault the cornea. Rather, this is due to application technique. The lens can be removed and reapplied.
Irregular Corneas
Troubleshooting for irregular corneas is fundamentally different compared to troubleshooting for normal corneas due to the shape and fit of the lens. The UltraHealth lens has a reverse geometry GP design built to vault the central cornea. Because of this, and to avoid application bubbles, the lens is applied by filling it with sterile saline solution. When diagnostically fitting an UltraHealth lens, use regular fluorescein; high-molecular-weight fluorescein is not required.
Comfort The most common problem responsible for decreased comfort is the GP portion bearing on the apex of a corneal irregularity (e.g., corneal ectasia, Salzmann’s nodular degeneration, scar, etc.). Patients will often describe this as decreased wear time or a dull ache after hours of wear. The Ultrahealth lens is somewhat dissimilar to a corneal GP lens in that there is no tolerance for a three-point-touch or apical bearing fitting relationship upon dispense. The lens must completely vault the cornea (optimally by 50μm to 100μm). This allows for some assumed settling over the wear time. You can achieve this during diagnostic fitting by applying successive vault value lenses until corneal clearance occurs (Figures 5 and 6). This is very similar to the apical clearance fitting procedure that was found to be the most advantageous in the Collaborative Longitudinal Evaluation of Keratoconus (CLEK) trials (Edrington et al, 1996).
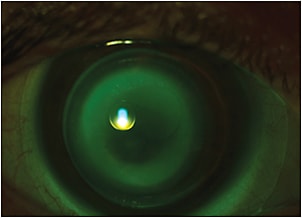
Figure 5. Central bearing of an UltraHealth lens on a keratoconic eye. The vault will need to be increased by roughly 100μm to vault the apex of the cone.
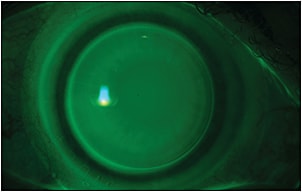
Figure 6. Optimal vault of an UltraHealth lens on a keratoconic eye. Note the even fluorescein pattern centrally. There is no darkening of fluorescein that would indicate bearing on the apex of the cone. The slightly darker band inside the junction is the inner landing zone where the partial weight of the GP lens rests on the cornea. More peripherally, there is edge lift of the GP portion (bright band). Outside of the junction, there is outer landing zone bearing where the SiHy skirt balances the weight of the lens against the eye (dark band).
Central bearing requires a higher-vault lens to correct. Do not steepen the skirt to raise the lens off of the cornea. The newly designed SiHy skirt will not be able to sustain that lift, and the lens will eventually fall back, or crash, onto the cornea.
If the lenses are very difficult to remove, this represents excessive vault or a skirt that is too steep (Figure 7). Excessive vault will cause seal off and will restrict the tear pump under the lens. However, most often, patients will have poor initial comfort with an excessively vaulting lens, indicating that a change is necessary.
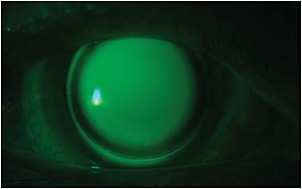
Figure 7. Excessive vault of an UltraHealth lens on a patient who has keratoconus. Aside from the deep green color of excessive fluorescein in the post-lens tear reservoir, the dense inner landing zone bearing is a clue that the lens has excessive vault. Differentiating between the excessive vaulting lens and the optimal vaulting lens (Figure 6) is possible by judging the location of the dark band. In the optimal vault, the dark band is outside of the junction (soft skirt bearing: desirable). In the excessive vaulting lens, the dark band is inside the junction (GP bearing: undesirable). Note that mild darkening at the inner landing zone is considered optimal. A dense band at the inner landing zone as pictured above is undesirable. This vault should be decreased by approximately 50μm.
Fitting Problems Some patients will complain of fluctuating vision and/or discomfort that, on the surface, do not appear to be a vault problem (e.g., lenses are comfortable on some days and uncomfortable on others). Close inspection of optical coherence tomography (OCT) images has identified a potential problem that is remedied by altering the application technique.
If a patient (or office staff) is applying UltraHealth lenses too forcefully, by pushing the lens onto the eye, excessive fluid will be forced from the bowl of the lens, and a vacuum will be created in the post-lens tear reservoir. This will, in turn, pull the lens too tightly onto the cornea and force the inner landing zone to indent the cornea. Remedy this problem by teaching the patient to allow the fluid in the lens to pull the lens onto the cornea during application. This “gentle” application technique prevents the vacuum of fluid, and the visual fluctuations and comfort problems will stop (Figure 8).
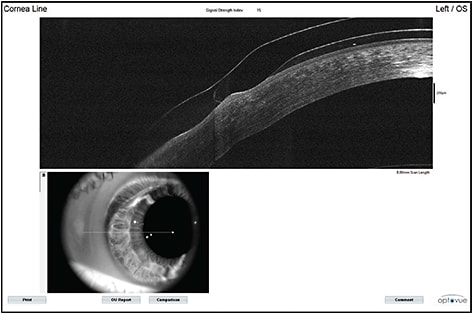
Figure 8a. An UltraHealth lens forcefully applied on a keratoconic eye. The inner landing zone is severely compressing the cornea. This patient complained of odd visual fluctuations and admitted to strongly forcing the lens onto the eye (in an attempt to avoid application bubbles).
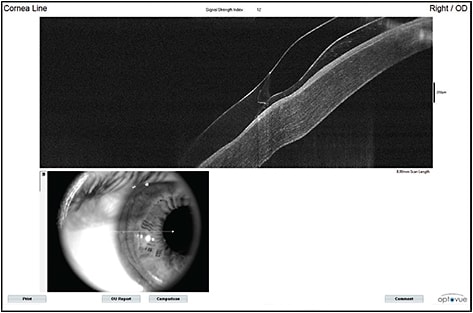
Figure 8b. The same lens after removal and reapplication with the “gentle” technique. The corneal area under the inner landing zone is still compressed from the weeks of warpage. However, there is now ample space under the inner landing zone. This patient practiced the “gentle” technique for several days and reported that his vision had completely stabilized.
If this does not fix the problem, it is likely that you are overvaulting the cornea and placing too much pressure on the inner landing zone. Decrease the vault by 50μm, and this problem will resolve.
Issues Noted in Both Normal and Irregular Corneas
White Deposit In some patients, after wearing lenses for four to six months, a white ring may develop in the soft skirt area of the lens (Figure 9). This is more prevalent in patients who have meibomian gland dysfunction or blepharitis. This substance has been tested and identified as a calcium salt. It is completely innocuous. If this is present at the six-month point, it is time to replace the lens anyway. If it is present after only a few months, we reassure these patients that there is no significant effect and use it as a springboard to discuss lid hygiene.
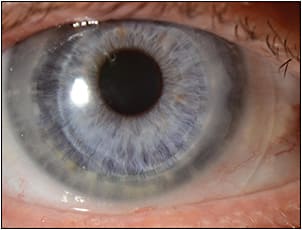
Figure 9. Keratoconic patient overwearing an UltraHealth lens for one year without replacement. A white deposit is visible on the soft skirt. Other than the odd appearance, this deposit is not harmful to the cornea and does not lead to any complications.
Soft Skirt Tearing Patients commonly ask about the potential of the soft skirt tearing away from the GP portion of the lens. Although this was quite common with the old SoftPerm and Saturn lenses, the SynergEyes lenses use a “Hyperbond” technology, in which the two materials are covalently bonded together. This junction will not split, tear, crack, or break. However, patients do occasionally report tears in the soft skirt at the lens periphery.
Skirt tears are always due to user error, and most often occur when patients are using fingernails to dislodge the lens. Proper removal technique involves breaking the capillary force of the soft skirt by pinching the superior or inferior skirt with the fleshy part of the finger tips and never the nails.
Impression Ring Some practitioners note an impression ring after removal of a Duette HD, Duette Progressive, or UltraHealth lens. This may result from the aforementioned forceful application or from a skirt that is too steep. In practice, only 1% to 2% of lenses ordered should be with the steep skirt. The vast majority should be ordered as a flat or flat 2 skirt.
Conclusions
The newest generation of hybrid lenses can offer your patients benefits that far surpass other lens modalities. For normal corneas, the Duette HD and Duette Progressive can give astigmatic or astigmatic presbyopic patients the cylinder correction that they need with superior and far more stable vision than with soft torics. For irregular corneas, the Ultrahealth lens has replaced corneal GPs as a first line lens for some practitioners.
With a minimal amount of skill, and the knowledge gained from fitters who have successfully used the lenses for years on hundreds of patients, every practitioner should feel comfortable fitting hybrid lenses. Knowing the simple troubleshooting techniques discussed here will make you much more confident in setting patient expectations and can help you take your success rate to the next level. CLS
For references, please visit www.clspectrum.com/references and click on document #226.
Note: The editorial policy of Contact Lens Spectrum is to generally report broadly about products, unless there is only one product or one company making products within a category.

|
Dr. Sonsino is in private practice in Nashville, Tenn. He is a diplomate in the Cornea, Contact Lenses, and Refractive Technologies section of the American Academy of Optometry. He is also a member of the American Optometric Association’s Council on Cornea and Contact Lenses, a fellow of the Scleral Lens Education Society, and is on the advisory board of the Gas Permeable Lens Institute. He is a consultant or advisor to Alcon, Optovue, SynergEyes, and Visionary Optics and has proprietary interest in LVR Technology. |