


Contact Lens Case Reports
Initial Selection of Corneal Versus Scleral GP Lens
BY PATRICK J. CAROLINE, FAAO, & MARK P. ANDRÉ, FAAO

Scleral lenses have dramatically changed the landscape of how we manage patients who have irregular corneas or ocular surface disease. Today, a primary question for both practitioners and students is: When is a patient a good candidate for a corneal GP lens, and when should that modality be abandoned for a scleral lens? Zheng et al addressed that question in a poster presented at the 2015 Global Specialty Lens Symposium titled “Corneal Elevation Differences and the Initial Selection of Corneal and Scleral Contact Lens.” The poster described a topographical technique that can help determine whether a patient who has irregular astigmatism might be best fitted with a corneal or a scleral lens design.
How the Technique Works
A topographer’s axial display map describes the dioptric power of the cornea, and it illustrates the shape and location of corneal astigmatism. However, it provides only limited information that can be used in fitting GP lenses. The elevation display, on the other hand, shows the relationship of a known spherical (or aspherical) surface to the cornea in which the highest areas of corneal elevation are represented as red, and the lowest depressions are represented as blue (Figure 1).
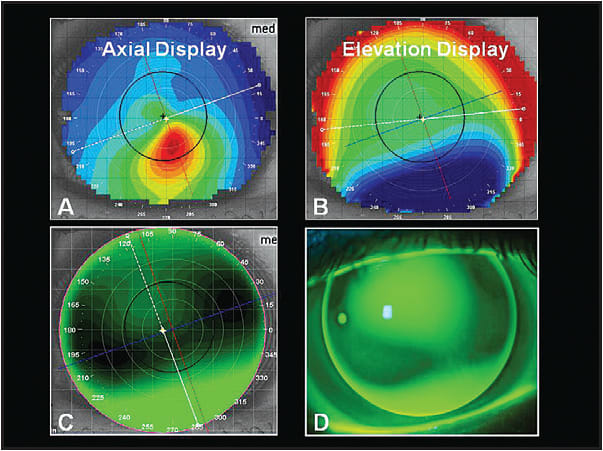
Figure 1. Axial display (A) of a patient who has moderate keratoconus. Note how the elevation display (B) better represents the simulated (C) and actual (D) corneal lens fluorescein pattern.
The authors retrospectively evaluated the display maps of 87 patients (126 eyes) to identify characteristics leading to either corneal GP success or failure. For each map, they determined the elevation change along the meridian of greatest elevation difference by rotating the topographer’s “section” scan, which shows the corneal elevation along an entire meridian (Figure 2).
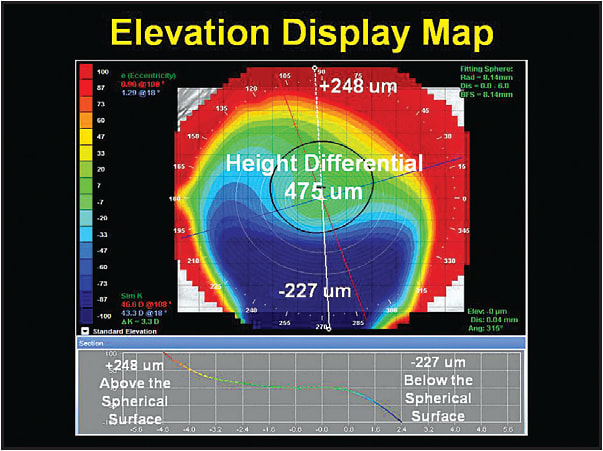
Figure 2. Rotating the section profile bar shows the elevation along the entire meridian and easily locates the meridian of greatest elevation change.
The results indicated that if a patient had less than 350µm of differential between the highest and lowest points along the greatest meridian of change, there was an 88.2% chance of the patient being successful with a corneal GP lens. The authors propose this as an acceptable clinical guideline when determining which type of GP lens to select for a patient (Figure 3). CLS
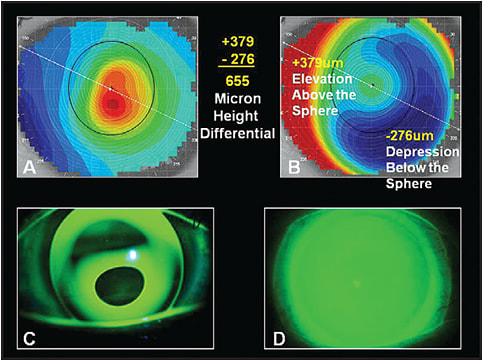
Figure 3. Axial map (A) and elevation map (B) of a patient who has advanced keratoconus (corneal elevation difference: 655µm) and the resulting corneal GP fit (C) and scleral lens fit (D).
For references, please visit www.clspectrum.com/references.asp and click on document #233.
Patrick Caroline is an associate professor of optometry at Pacific University. He is also a consultant for Contamac. Mark André is an associate professor of optometry at Pacific University. He is also a consultant for CooperVision.