


Refractive Focus
Quantifying Subjective Assessment of Visual Quality
BY JASON MARSACK, PHD

Readers of Contact Lens Spectrum are intimately familiar with the most common methods for assessing visual performance: visual acuity measurements. These measurements are easy to perform using visual acuity charts, making it feasible to quantify vision in the presence of a given correction, to compare two corrections, and to identify a change in vision over time, etc.
But what is truly measured with visual acuity is best described as a quantity of vision, and many factors beyond quantity of vision are equally important to contact lens patients. Lens discomfort, handling issues, and a host of other factors can influence the overall experience associated with wearing a contact lens and can result in cessation of lens wear (Dumbleton et al, 2013). Historically, these qualitative aspects that influence lens wear have been more challenging to measure compared to a quantitative variable such as visual acuity, but progress is being made to transform subjective information into quantitative data that can be used in evaluating lens performance.
Using a Visual Analog Scale to Quantify Contact Lens Performance
The focus of this article will be on one such method: the visual analog scale. Crichton (2001) describes the visual analog scale as “a measurement instrument that tries to measure a characteristic or attitude that is believed to range across a continuum of values and cannot easily be directly measured.” Such a description could be readily used to describe contact lens-related complications such as discomfort and dryness, or it can be applied to the subjective assessment of visual quality.
Whether talking about discomfort, dryness, or visual quality, a patient is likely to provide a subjective response. In a practical sense, the visual analog scale attempts to project this subjective response onto a line of a known length (e.g., 10cm is common) with anchoring descriptors on both ends of the line. The patients’ task is to indicate the point between these two descriptors on the continuum that best conveys their assessment of the subjective variable under investigation. Figure 1 shows an example as adapted from Davies et al (1992).
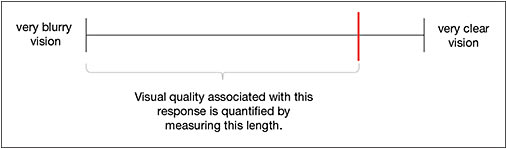
Figure 1. Example based on the visual analog scale described in Davies et al (1992). The red line indicates the patient’s perceived visual quality on the visual analog scale in response to the question “Using the end points that are marked as guides, how would you rate overall visual quality with the lenses that you are currently wearing?” The line is closer to the clear end of the spectrum than to the blurry end of the spectrum, and the length of the line can be measured. The question and descriptive anchors could be modified to assess a variable such as comfort. (Note that in the Davies study, the visual analog scales were oriented vertically).
Examples of the Visual Analog Scale in the Vision Literature
Investigators have utilized the visual analog scale when evaluating visual performance in the presence of an ophthalmic correction. Following are several examples from the literature.
How well does visual acuity predict visual quality? Davies et al (1992) used the visual analog scale to demonstrate that having good visual acuity does not necessarily correlate with having good visual quality. In their study, they measured visual acuity and asked subjects to indicate their perceived visual quality on a visual analog scale. The resulting correlation coefficients relating visual quantity (acuity) and quality were weak (~0.59 for high-contrast and ~0.51 for low-contrast acuity).
How happy are patients with scleral contact lens correction? Visser et al (2001) utilized a 100mm visual analog scale to rate several dimensions of satisfaction associated with scleral contact lens wear. When stratified by subject diagnosis, the median score for visual quality associated with keratoconus subjects was 75/100, whereas the rating for overall satisfaction of the lens was 84/100. While the numbers in isolation may be somewhat challenging to interpret, when comparing them to each other (75 versus 84) it may be hypothesized that non-visual factors are integral to satisfaction with the lenses.
How well can patients report blurriness in their vision? Kollbaum et al (2012) utilized a visual analog scale to assess subjects’ perceived visual quality in the presence of blurring spectacle lenses of different powers, ranging from –0.50D to +1.50D.
In this experiment, the investigators found a mean dioptric width of the predicted 95% confidence interval across the levels of blur of 0.21D using the visual analog scale, demonstrating that it can detect blur under 0.25D.
This work was also important in that it compared the performance of the visual analog scale to that of two additional techniques for quantifying subjective information: the numeric rating scale and the categorical rating scale.
Integrating Subjective and Objective Information
By quantifying data that have historically been reported in a qualitative nature, clinicians and researchers gain additional insight into the performance of an ophthalmic correction. While this prospect is exciting, interpreting the values associated with the visual analog scale can be challenging.
As Crichton (2001) stated, when analyzing these results, many researchers tend to use the scales to measure change within an individual, and they rely on methods of analysis that tend toward rank ordering, which lessens the influence of the actual visual analog scores.
Summary
In trying to answer the question, “How do we know whether a contact lens is providing good visual quality?” it is clear that standard objective measures such as acuity need to be augmented by methods to quantify aspects of contact lens wear that have traditionally been elusive. Tools such as the visual analog scale may give clinicians and researchers additional ways of assessing a patient’s perceived performance of the lens. This may also allow quantitative evaluation to be personalized to the aspects of lens wear most important to each patient. CLS
For references, please visit www.clspectrum.com/references and click on document #231.
Dr. Marsack completed a PhD in Physiological Optics and Vision Science at The University of Houston, College of Optometry, where he is currently a member of the faculty. He conducts independent research as well as research within the Visual Optics Institute and The Ocular Surface Institute. His research interests include optical aberration of the eye, custom and pseudo-custom correction of optical aberration, visual performance, metrics predictive of visual performance, and ocular drug delivery.