


CONTROVERSIES IN CARE
Controversies in Contact Lens Care
A comparison of survey results from a recent AOA event to current evidence-based outcomes.
By Thomas G. Quinn Jr., OD, MS; Jeffrey J. Walline, OD, PhD; Jeffrey Sonsino, OD; Edward S. Bennett, OD, MSEd; Shalu Pal, OD; Glenda B. Secor, OD; & Randall F. Fuerst, OD
Rapidly evolving technology and knowledge have created excitement—and some controversy—in the contact lens arena. The American Optometric Association (AOA) Contact Lens and Cornea Section (CLCS) presented an interactive program “Controversies in Contact Lens Care” at the 2014 Optometry’s Meeting in Philadelphia.
During the event, audience members were polled prior to the presentation of information on 12 very popular and controversial areas. Audience responses were then compared to current evidence-based outcomes on topics such as myopia control, contact lens care and replacement, case care, scleral lenses, and presbyopic preferences. This insight can potentially assist the Council in the development of new ideas for future programs because not all audience responses were predictable.
We also believe that the Contact Lens Spectrum readership would benefit from learning about the results from this program and their implications.
1. What myopia control method do you prescribe most often?
Bifocal or multifocal spectacles, orthokeratology, and soft bifocal contact lenses were the three most-prescribed types of myopia control by polled practitioners (Figure 1). While orthokeratology (Charm and Cho, 2013; Chen and Cho, 2012; Cho and Cheung, 2012; Cho et al, 2005; and others. Full list available at www.clspectrum.com/references.) and soft bifocal contact lenses (Aller and Wildsoet, 2006; Anstice and Phillips, 2011; Lam et al, 2014; Sankaridurg et al, 2011; and others) have been found to slow the progression of myopia in children, soft multifocal or bifocal spectacles have never slowed the progression of myopia by more than 34% (Berntsen et al, 2012; Cheng et al, 2014; Correction of Myopia Evaluation Trial [COMET] 2 Study Group for the Pediatric Eye Disease Investigator Group, 2011; Edwards et al, 2002; and others), even in esophoric patients who have high accommodative lag and are most expected to benefit from multifocals (Berntsen et al, 2012; COMET 2 Study Group, 2011; Fulk et al, 2000).
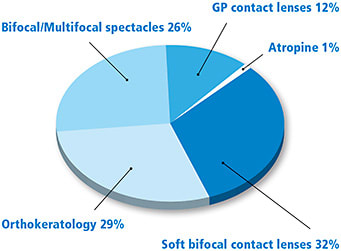
Figure 1. Proportion of audience who chose each myopia control method as the one they prescribe most often.
No participants reported using atropine for myopia control, but low concentrations of atropine have recently been shown to slow myopia progression (Chia et al, 2012; Chia et al, 2014; Wu et al, 2011) and even to prevent the onset of myopia (Fang et al, 2010). Importantly, these patients had few complaints of symptoms associated with mydriasis or cycloplegia. Although none of these treatments is approved by the U.S. Food and Drug Administration (FDA) for myopia control, they should be considered when trying to slow the progression of myopia in children.
2. Do you recommend that patients clean their contact lens cases every day?
Despite the fact that poor contact lens case hygiene has been shown to increase the risk of microbial keratitis by nearly four times (Stapleton et al, 2012), only half of the optometrists in attendance recommend that their patients clean the case daily.
The most effective way to reduce the number of microbes on a contact lens case is to fill it 80% with multipurpose solution, rub it for five seconds with the finger, wipe it dry with a tissue, then air dry the case upside down on a clean tissue (Wu et al, 2011). These steps should be verbalized, demonstrated, and provided in written form to reduce patients’ risk of serious contact lens complications. In fact, patients who receive both written and verbal instructions regarding contact lens case care are less likely to have cases that are contaminated by bacteria (Tilia et al, 2014).
3. How often do you tell your patients to replace their contact lens case?
The majority of attendees indicated that they recommend patients replace their contact lens case every three months (56%) (Figure 2). The second most common response (24%) was to recommend case replacement with every new bottle of disinfecting solution. Only 13 percent recommended monthly case replacement. Very few (4% and 2%, respectively) indicated that they don’t recommend a replacement schedule or that they recommend annual case replacement.
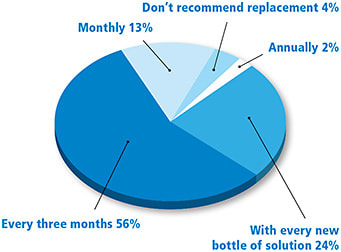
Figure 2. Proportion of audience who chose each schedule of contact lens case replacement.
Studies have found that replacing the contact lens case every six months or less often increases the risk of moderate and severe microbial keratitis 5.4 times compared to replacement every three months (Stapleton et al, 2012).
There is also evidence that cases may develop significant contamination after two weeks of use (Lakkis et al, 2009), suggesting that case replacement at least monthly would be advisable.
4. What contact lens replacement schedule do you prescribe most often?
Annual lenses were not an option for our practitioners attending this presentation. Monthly disposable lenses are prescribed at twice the rate of the other options (Figure 3).
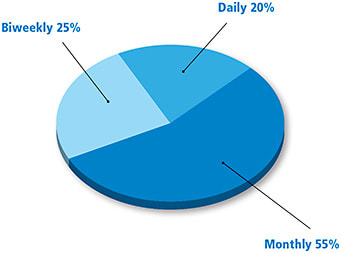
Figure 3. Proportion of audience who prescribe each replacement schedule most often.
National studies for 2013 conducted by ABB Optical and GfK Retail and Technology are almost identical in their findings. They show that only 1% of practitioners still prescribe conventional lenses. Two-week and monthly replacement lenses are being prescribed at an equal rate of 36% to 41% (Nichols, 2014). Monthly lenses are less frequently prescribed, and daily disposable lenses have a higher prescription rate than that prescribed by our audience of practitioners. The Contact Lens Spectrum annual survey results are very similar to the trends seen at the summit. The recommendation of daily disposable lenses is predicted to increase in 2015 (Nichols, 2014).
5. When prescribing contact lenses, do you consider UV protection?
Two-thirds of our audience practitioners do not consider ultraviolet (UV) protection when prescribing contact lenses. Only 11% always consider UV protection when prescribing lenses, and 22% occasionally consider UV protection.
We are all aware of the damage that UV light can do to the eye, including macular, retinal, lenticular, corneal, and scleral damage. UV-blocking sunglasses still allow up to 45% of UV peripheral rays to reach the eye. UV-blocking contact lenses can help block these peripheral rays (Kwok et al, 2003; Walsh et al, 2001).
UV damage is cumulative over the course of our life, with 50% of that damage occurring before the age of 20 (Green et al, 2011). By age 15, 80% of Australian children have signs of UV damage (Ooi et al, 2006). Only 3% of our children wear sun protection outdoors, so practitioners need to do a better job of educating parents about the harmful effects of UV radiation (Young and Sands, 1998). Maximum protection is achieved with UV-blocking contact lenses, UV-blocking sunglasses, and by wearing a wide-brimmed hat (Young and Sands, 1998).
6. Do you pair specific contact lenses and care solutions when prescribing?
There is evidence that some care solution-lens material combinations are more likely to result in corneal staining, discomfort, and corneal inflammatory events (Carnt et al, 2009), and the Andrasko Staining Grid (www.staininggrid.com) shows that some contact lens solution and lens material combinations are more likely to result in corneal staining after two hours. In spite of this, the majority of respondents prescribed the same care solution regardless of material (Figure 4). Only 17% of the respondents use the Andrasko Staining Grid when deciding what care regimen to use for a specific lens material. It is important to note that the FDA specifically states that contact lens care solutions can cause serious problems—including eye infections—if not used correctly (FDA, 2014).
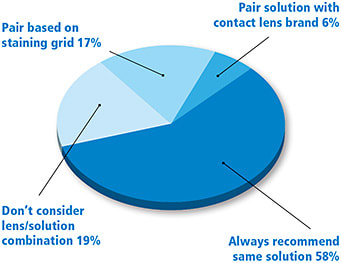
Figure 4. Proportion of audience who pair contact lenses and care solutions based on various strategies.
7. When do you recommend a part-time contact lens wearer dispose of 30-day lenses?
This is a relatively common question from patients, and the spread of responses suggests that it’s a difficult one to answer. Nearly half of the respondents (49%) recommend that part-time wearers of a monthly lens replace their lenses 30 days after the foil pack is opened. The remaining respondents were fairly evenly divided between recommending lenses be replaced after 30 days of actual wear (24%) and refitting occasional wearers into daily disposable lenses (27%).
The question here is, “What happens to the contact lens while it is sitting in a case waiting to be worn?” Contact lens storage case contamination occurs in 30% to 85% of cases (Szczotka-Flynn et al, 2010; Gray et al, 1995; Devonshire et al, 1993; Yung et al, 2007; and others). Bacteria in the case may form a biofilm, which is easily removed initially but is significantly more resistant over time (Farber et al, 1995; Szczotka-Flynn et al, 2009). In fact, as mentioned previously, storage cases may become contaminated after only two weeks (Lakkis et al, 2009).
Time works against safety in another regard as well. Soaking lenses in disinfecting solution may not be sufficient to adequately eliminate the risk of microbial contamination of lenses (Wu et al, 2010; Dart, 1997; Wilson et al, 1991). Lens materials and contact lens care solutions interact, which can reduce disinfection ability (Santos et al, 2011).
The safest option, particularly for occasional lens wearers, is to be refit into daily disposable lenses, as daily disposables have been shown to reduce the risk of severe microbial keratitis compared to reusable lenses (Dart et al, 2008).
8. What replacement modality do you prescribe most frequently to optimize compliance?
An overwhelming 73% of respondents prescribe daily disposable contact lenses to improve compliance. Eighteen percent of respondents say that they optimize compliance with monthly replacement, and 10% with two-week replacement. Although most of our colleagues believe that daily replacement of lenses has the best compliance rate among our patients, there are still problems with compliance.
Dumbleton et al (2013) surveyed 2,147 respondents asking for compliance rates with recommended replacement schedule. They reported compliance rates for two-week replacement (34%), daily disposables (74%), and one-month replacement (67%). Even with the daily disposable modality, one-fourth of patients do not adhere to the recommended replacement schedule.
In Japan, an area of the world that many of us believe has a strong cultural basis for compliance, there are still problems with patient adherence to lens replacement schedules. Ichijima et al (2014) found that the most commonly prescribed contact lens modalities were two-week replacement (32.1%) and daily disposable (31.0%). Of those two modalities, only 42.7% of patients adhered to the recommended replacement schedules.
9. In your practice, how often do you fit full scleral lenses (>16.0mm)?
When polled about the reason for fitting scleral lenses, 64% of audience members reported not fitting scleral lenses at all. Approximately one-fourth fit scleral lenses for irregular corneas only (Figure 5). Very few respondents were fitting sclerals for irregular corneas and healthy astigmatic single-vision patients (5%). Likewise, very few respondents were fitting for irregular corneas and healthy astigmatic presbyopic patients (5%).
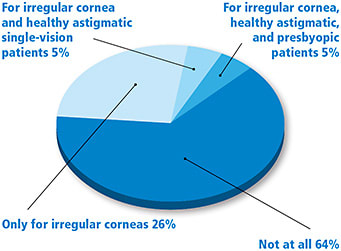
Figure 5. Proportion of the audience that reports fitting scleral lenses with diameter of >16.0mm.
Far more publications reference fitting scleral lenses on irregular corneas compared to fitting them on normal corneas. Michaud (2014) wonders whether scleral lenses are safe enough for normal corneas. To prevent corneal swelling, scleral lenses must sufficiently vault over the cornea and be thin enough to allow adequate oxygen transmission (Compañ et al, 2014).
10. What is the average number of visits it takes you to fit a full scleral lens (>16.0mm)?
In terms of the logistics of fitting scleral lenses, 65% of respondents were able to achieve a final fit within three to five visits. The remaining respondents were split between one to two visits and three to four visits. This agrees with a retrospective chart review at Mayo Clinic in which the average number of visits required to achieve optimal scleral lens fit was three, with a range of two to six visits (Schornack et al, 2014). A similar study at the University of California-Davis reported an average of 6.2 visits necessary for fitting (Pecego et al, 2012).
11. What is the healthiest (least infections and other complications requiring temporary discontinuation of lens wear) form of contact lens?
There was a clear trend from the respondents that is consistent with the literature. The two most healthy lens modalities are daily disposable (68%) and GP contact lenses (28%). A total of 6% of the respondents were split between silicone hydrogel and hydrogel contact lenses worn for one month on a daily wear basis.
The use of daily disposable lenses has greatly increased in the United States in the last three years from 15% in 2010 to 31% in 2013; internationally, daily disposable lens use only increased from 29% to 31% over that same period (Morgan et al, 2011; Morgan et al, 2014).
Daily disposable lenses have the lowest complication rate when compared to other lens modalities (Henry and DeKinder, 2014), and they result in fewer unscheduled office visits as well as improved visual acuity, comfort, and patient satisfaction (Hamano et al, 1994; Freeman et al, 1997; Nason et al, 1994). These patients are also more compliant with contact lens replacement compared to those using monthly and two-week replacement schedules (Dumbleton et al, 2009).
GP lenses also resulted in a low incidence of complications. Stapleton et al (2008) reported that the risk of eye infection was lowest with GP wearers (1.2 per 10,000 wearers), followed by daily wear soft lens wearers (1.9 per 10,000 wearers) and daily disposable soft lens wearers (2.0 per 10,000 wearers). GP lenses also demonstrate advantages in quality of vision and eye health (Santos et al, 2011; Stapleton et al, 2008; Cavanagh et al, 2009; Forister et al, 2009; and others).
Despite three to five times greater oxygen transmission for silicone hydrogel compared to hydrogel materials, there is no reduced risk of eye infection with silicone hydrogel lens wear, notably in extended wear (Stapleton et al, 2008; Schein et al, 2005). However, there is less induced corneal swelling than with hydrogel lenses, so they may reduce the risk of hypoxic complications (Jalbert et al, 2009).
12. For a spherical soft lens wearer who is now presbyopic, which option do you prefer?
Audience members primarily prefer to fit soft multifocal contact lenses on presbyopic patients (Figure 6). This reflects the gradual transition from monovision to multifocals as the practitioner preference.
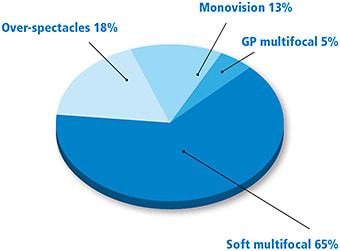
Figure 6. Proportion of audience who preferred a particular modality when fitting presbyopic patients.
In an annual survey of practitioners compiled by Contact Lens Spectrum, 72% of presbyopes wearing contact lenses preferred multifocals (versus 59% in 2008), 19% preferred monovision (versus 27% in 2008), and 8% preferred using single-vision lenses and over-spectacles (versus 14% in 2008) (Nichols, 2014; Nichols, 2009). Approximately 68% to 76% of people prefer multifocal to monovision contact lenses (Kirschen et al, 1999; Situ et al, 2003; Richdale et al, 2006; Benjamin, 2007; and others).
Monovision contact lens wearers experience greater monocular suppression of blur with increasing add power, greater loss of contrast sensitivity, and more compromise on critical vision tasks compared to soft multifocal contact lens wearers (Kirschen et al, 1999; Richdale et al, 2006; Fernandes et al, 2013; Rajagopalan et al, 2006). Furthermore, anisometropia increases by 0.50D or more in 29% of monovision wearers (Jain et al, 1996).
The selection of soft multifocals—versus GP multifocals—makes sense because most patients are satisfied spherical soft lens wearers. Nevertheless, if satisfactory vision is not achieved with soft multifocals, GP multifocal lenses represent a viable option, and they result in better quality of vision compared to soft multifocal lenses and monovision lenses (Rajagopalan et al, 2006).
Summary
The responses to these controversial contact lens topics should help optimize patient care and success. The consumer website www.contactlenssafety.org, which includes 50 commonly asked questions and evidence-based answers pertaining to contact lens safety, can also be a very beneficial resource to practitioners. This website represents a cooperation between the AOA CLCS and the American Academy of Optometry’s Cornea, Contact Lenses, and Refractive Technologies Section. CLS
The authors would like to acknowledge Dr. Harvard Sylvan and CooperVision for their support of this program.
For references, please visit www.clspectrum.com/references and click on document #230.
Dr. Quinn is in group practice in Athens, Ohio. He is an advisor to the GP Lens Institute (GPLI) and an area manager for Vision Source. He is an advisor or consultant to Alcon and B+L, has received research funding from Alcon, AMO, Allergan, and B+L, and has received lecture or authorship honoraria from Alcon, B+L, CooperVision, GPLI, SynergEyes, and STAPLE program. You can reach him at tgquinn5@gmail.com. | |
Dr. Walline is an associate professor at The Ohio State University College of Optometry. He has received research funding from Johnson & Johnson Vision Care. You can reach him at walline.1@osu.edu. | |
Dr. Sonsino is in private practice in Nashville, Tenn. He is a diplomate in the Cornea, Contact Lenses, and Refractive Technologies section of the American Academy of Optometry (AAO). He is also a member of the American Optometric Association’s (AOA) Council on Cornea and Contact Lenses, a fellow of the Scleral Lens Education Society, and is on the advisory board of the GPLI. He is a consultant or advisor to Alcon, Optovue, SynergEyes, and Visionary Optics and has proprietary interest in LVR Technology. | |
Dr. Bennett is assistant dean for Student Services and Alumni Relations at the University of Missouri-St. Louis College of Optometry and is executive director of the GPLI. You can reach him at ebennett@umsl.edu. | |
Dr. Pal is in a solo practice in Toronto. She is a member of the AOA Contact Lens and Cornea Section Council, chair of the AOA Student & New Graduate Committee, a member of the CAO, and on the Continuing Education committee of the Ontario Association of Optometrists. She is a speaker, writer, or consultant for Allergan, Alcon, B+L, CooperVision, J&J, Menicon, Novartis, and TruForm Optics. | |
Dr. Secor is in private practice in Huntington Beach, CA. A Fellow of the AAO and Diplomate of the Cornea and Contact Lens Section, she is a past chair of this section. She has been a consultant to Alcon. | |
Dr. Fuerst is a partner in a three-office, eight-doctor practice in Sacramento, CA. He is the immediate past chair, AOA Contact Lens and Cornea Section, and serves on advisory boards of several ophthalmic companies. He has received travel funding from Alcon, B+L, BioTissue, and SynergEyes. |