


Reader and Industry Forum
Integrating Current Thoughts on Myopia Control
BY JEFFREY KROHN, OD, FAAO, & MOSHE SCHWARTZ, OD, FAAO

The rate of myopia in the United States has been climbing rapidly in the past 40 years from 25% to 42% of the population (Sperduto et al, 2009). Are we, as eyecare providers, adequately engaging with our patients and community regarding this condition? Perhaps it is time that we assert some control over this potential epidemic. Considering the incidence rate and current progression, it is crucial to assess when is the appropriate time to initiate treatment. Our obligation and commitment to our patients starts from their initial well visit (usually around the age of 3).
Initiate discussions about myopia control prior to its development through education about changes to lifestyle and habits (Guggenheim et al, 2012; Sherwin et al, 2012; Lim et al, 2010). Approaching myopia control as a treatment protocol rather than as a compensation for refractive error is an essential step in partnering with our patients and their parents.
Start When They Are Young
There are many modalities available in myopia control, including contact lenses, pharmaceuticals, spectacle lenses, and behavioral modification. Introducing contact lenses to pediatric patients can be professionally, financially, and personally rewarding. While practitioners might be initially apprehensive about fitting pediatric patients with contact lenses for myopia control due to perceived complexity and chair time, that apprehension in unfounded.
In fact, the Contact Lenses in Pediatrics (CLIP) study (Walline et al, Sept. 2007) showed that the main difference between pediatric and teenage patients was in the training of lens application and removal; the training took 15 minutes longer in the pediatric patients compared to teenagers. Further bolstering the confidence of practitioners to get involved, the Pediatric Refractive Error Profile (PREP) study (Walline et al, Nov. 2007) supports the observation that contact lenses improve children’s and teenagers’ perceived quality of life. Based on these studies, contact lenses should soon become the standard of care for managing refractive status and myopia control.
Peripheral Blur Issues
Prescribing spectacle lenses in an attempt to halt myopia progression has been extensively studied, with recent findings showing that bifocal spectacles and prismatic bifocals somewhat reduced the progression of myopia (0.81D to 1.05D, respectively) (Cheng et al, 2014). While original notions or beliefs were that the add power in the spectacle prescription would reduce myopia progression due to accommodative control, it is rather important to emphasize that the add power is effective through the creation of peripheral blur (Smith et al, 2005; Smith, 2011).
Hyperopic blur shifts the image from behind the retina and brings it anteriorly at the periphery. Other correction modalities cause myopic blur in the periphery, which encourages axial elongation, increasing overall myopia.
However, practitioners should not discount the importance of accommodative testing and accommodative dysfunction in the care of young people who have myopia. It is important to perform extensive near testing on all emerging myopic patients and to address their accommodative state. It is also speculated that the “mechanical tension created by the crystalline lens or the ciliary body restricts equatorial ocular expansion and causes accelerated axial elongation,” consequently leading to larger-than-average eye size in children at risk for myopia (Berntsen et al, 2010).
Shifting the focal points in the peripheral retina has opened the doors to multiple approaches of myopia control. These can (and should) fit into any eyecare practice under the sub-specialty of “Myopia Control Services,” whether through bifocal spectacle correction, multifocal contact lenses, or corneal reshaping.
Multifocal contact lenses, available as either standard frequent replacement lenses or as customized lenses, show great promise. In particular, custom lenses allow practitioners to control the optic zone diameter. When the contact lenses can be designed to address patients’ pupil size and desired add power, while also specifying a transition of the add power, then laboratories and practitioners begin to truly engage in precision management of peripheral blur.
Corneal Reshaping
Corneal reshaping has demonstrated great promise in controlling axial length and hindering myopia progression as a treatment modality (Cho and Cheung, 2012; Hiraoka et al, 2012). This modality uses a reverse geometry GP lens design (Figure 1) to exert central pressure and paracentral “pulling,” which leads to central flattening and peripheral steepening. The result is lower central myopia (better uncorrected vision) and peripheral retinal hyperopia, thus delivering immediate and long-term positive results.
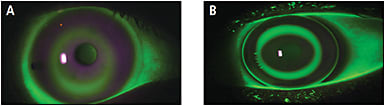
Figure 1. The goal of any reshaping contact lens design is to achieve perfect centration and a “bull’s eye” fluorescein pattern. There is, in essence, no difference in the fluorescein pattern between scleral (A) and corneal (B) reshaping lenses.
Corneal reshaping lenses are currently available through a number of manufacturers, each with their own proprietary designs. Practitioners must complete an online certification process before they can fit corneal reshaping lenses; two certification programs are available, depending on which corneal reshaping lenses practitioners wish to fit.
The availability of high-oxygen-permeability GP polymers allows these lenses to be safely worn overnight, with daytime “no lens” convenience. While there have been reports of tragic infections with overnight lens wear in corneal reshaping, recent studies show that these lenses do not increase the risk of microbial keratitis versus other overnight modalities of contact lens wear (Watt and Swarbrick, 2005).
Benefits to Your Practice
In today’s hectic practice, with the pressures that come with managed health care and the ever-present threat of diminishing returns on our services, incorporating myopia control can be highly rewarding in many ways. In particular, implementing a program including soft multifocal lenses or corneal reshaping can build patient loyalty and patient satisfaction while expanding our scope of practice through specialty services.
Addressing myopia as only a refractive state of the eye is a mistake whose significance is growing in importance. Myopia ought to be considered a medical condition to arrest and treat rather than something to compensate for with lenses; reducing final axial length is a very important goal and is now possible.
There is a direct correlation between high myopia and retinal detachment (Schepens and Marden, 1966; Kaluzny, 1970; Wilkinson et al, 1997), glaucoma (Perkins, 1979), and myopic macular degeneration (Chen et al, 2012; Saw et al, 1996); it is our obligation as caretakers of eye health to care for our patients diligently from the youngest age with proper education and services. CLS
For references, please visit www.clspectrum.com/references and click on document #232.
Dr. Schwartz practices in Specialty Contact lens practice in Owings Mills, MD. He is a Diplomate in the Cornea, Contact Lenses and Refractive Technologies section of the American Academy of Optometry (AAO). Dr. Schwartz is a consultant to Menicon USA and SpecialEyes and has received lecture or authorship honoraria from SpecialEyes. Dr. Krohn practices in Fresno, CA. He is a Diplomate in the Cornea, Contact Lenses and Refractive Technologies section of the AAO and is a regional administrator with Vision Source.