


POST-OP FITTINGS
Postoperative Contact Lens Fittings
The specifics of fitting contact lenses post-corneal collagen cross-linking and intrastromal corneal ring segment implantation.
By Melanie Frogozo, OD, FAAO
Keratoconus, pellucid marginal degeneration, and iatrogenic corneal ectasia secondary to laser refractive surgery are all characterized by progressive corneal steepening. In these non-inflammatory ectasias, the cornea assumes an asymmetrical contour, which leads to high irregular astigmatism and decreased visual acuity. For such conditions, corneal collagen cross-linking (CXL) and intrastromal corneal ring segment (ICRS) implantation are both well-accepted and widely performed treatment options.
Although CXL and ICRS implantation—both U.S. Food and Drug Administration (FDA)-approved procedures—are both effective in treating corneal ectasias, most patients who have undergone these surgeries need to wear contact lenses to reach their full visual potential. Therefore, it is important to become familiar with how these procedures change the corneal contour and, thus, the approach to fitting contact lenses postoperatively. This article will review contact lens fitting after CXL and ICRS implantation.
Procedures and Corneal Shape Changes
In patients who have primary and secondary ectasias, CXL and ICRSs help normalize the corneal contour and make it more optically regular. Nonetheless, the corneal shape is affected differently after each procedure. Understanding both procedures and the consequential postoperative corneal shape is therefore key to successful contact lens fitting in this population.
Corneal Cross-Linking CXL is a technique that uses ultraviolet light and a photosensitizer to strengthen the corneal stroma. The primary objective of CXL is to stop the progression of ectasia by enhancing the mechanical stability of the corneal tissue. Therefore, the best candidates for CXL are those who have documented progressive ectasia.
CXL is accomplished through a polymerization reaction as a result of combining riboflavin and ultraviolet A (UVA) irradiation. Riboflavin acts a photosensitizer and, when combined with UVA, increases the crosslinks between and within the corneal collagen fibers (Spörl et al, 1997; Ziaei et al, 2015). This interaction between riboflavin and UVA creates reactive oxygen species that promote the formation of covalent bonds between collagen fibers, increasing corneal rigidity, collagen fiber thickness, and resistance to enzymatic degradation. Additionally, the increase in overall strength of the cornea decreases stromal swelling and permeability in the anterior stroma (Spoerl et al, 1998; Wollensak, Spoerl, Seiler et al, 2003).
Interestingly, CXL is being investigated for other applications, such as treatment of non-responding infective keratitis (Alio et al, 2013), bullous keratopathy (Ghanem et al, 2010), and prevention of ectasia in refractive surgeries (Nguyen and Chuck, 2013). Figure 1 shows a patient undergoing the CXL procedure.

Figure 1. Patient undergoing a CXL procedure. Photo courtesy of Gregory Parkhurst, MD.
The basic CXL treatment protocol starts with de-epithelialization of the corneal surface followed by the stromal application of 0.1% isotonic riboflavin solution in 20% dextran. The riboflavin increases UVA absorption and prevents the corneal endothelium, lens, and retina from being damaged by UVA light. Note: to avoid UVA endothelial damage, the cornea must be at least 400 microns thick. Finally, UVA light at the wavelength of 360nm to 370nm with an accumulated irradiance of 5.4 J/cm2 is applied to the corneal surface for 30 minutes (Spoerl et al, 2003; Wollensak, Spoerl, Seiler et al, 2003).
Currently, attempts at bettering the basic protocol are being investigated. This research includes improving the stromal penetration of riboflavin while preserving the integrity of epithelium (Bikbova and Bikbov, 2014) and decreasing the amount of time that the patient is exposed to UV irradiation (Waszczykowska and Jurowski, 2015).
CXL changes the corneal shape by decreasing keratometric values. In patients who have progressive keratoconus, reduction in maximum keratometric values range from 1.45D to 6.16D, with an average of about 2.00D (Wollensak, Spoerl, and Seiler, 2003; Vinciguerra et al, 2009; Wittig-Silva et al, 2008). In comparison, those who have iatrogenic corneal ectasia after laser-assisted in situ keratomileusis (LASIK) only showed a reduction of 1.00D in their maximum keratometric value after CXL.
The variation in treatment response effectiveness may be due to the difference in riboflavin diffusion rates or the intrinsic pathophysiology of each individual disease (Hersh et al, 2011). Although there is mild flattening of the keratometric values from CXL, the overall shape change is not dramatically affected after the procedure. Thus, contact lenses can be fitted in a regular fashion post-CXL.
Intrastromal Corneal Ring Segments ICRS implantation is a surgical technique in which polymethyl methacrylate (PMMA) semi rings are implanted into the stroma to create central corneal flattening, which consequently reduces refractive error. Originally used for treatment of low myopia, ICRSs are currently used to improve vision in corneal thinning disorders, such as keratoconus and LASIK-induced corneal ectasia. ICRSs can also be offered as an alternative to corneal transplantation (Rabinowitz, 2010; Rabinowitz, 2013).
The ICRS procedure is reversible, and the segments can be removed. Once removed, the cornea appears to return to its pre-operative shape (Nosè et al, 1993). Figure 2 shows a patient after ICRS implantation in the left eye.
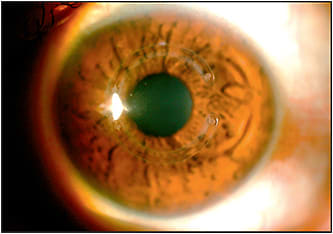
Figure 2. Keratoconic left eye after ICRS implantation.
The basic procedure of ICRS implantation starts with creation of a tunnel for the segments either via femtosecond laser or with a mechanical spreader provided by the manufacturer. The tunnel incision is usually 70% of the corneal thickness. After the tunnel is created, the plastic segments are placed within the stroma, and a suture is inserted to close the wound site.
Ideal candidates for ICRSs are patients who have mild-to-moderate ectasia and are contact lens-intolerant. Those considering ICRS must have a clear visual axis, a steepest keratometry value of ≤58D, and a corneal thickness at the insertion zone for the segment of at least 450 microns (Rabinowitz, 2010; Rabinowitz, 2013).
Placement location and combination of ICRSs used can vary depending on the type of ectasia being treated. Usually, implantation of smaller arc segments and greater width sizes leads to greater reduction in myopia. Customarily, an oval central cone is treated by implanting asymmetric segments: a wider segment inferiorly and a smaller width superiorly. In milder cases of keratoconus (in which the cone does not cross the horizontal meridian) and in cases of post-LASIK ectasia, a single inferior segment is used for treatment (Rabinowitz, 2010; Rabinowitz, 2013).
On average, ICRSs flatten the cornea by 2.0D to 3.0D, which is accompanied by two to three lines of gained best-corrected vision. Interestingly, improvement in best-corrected vision is thought to be due to a decrease in higher-order aberrations resulting from ICRSs (Rabinowitz, 2010; Rabinowitz, 2013).
Figure 3A shows a sagittal (axial) curvature map of a patient pre-ICRS implantation and post-implantation in the right eye. In this case, the max K decreased by 2.3D within an eight-month follow-up period (Figure 3B).
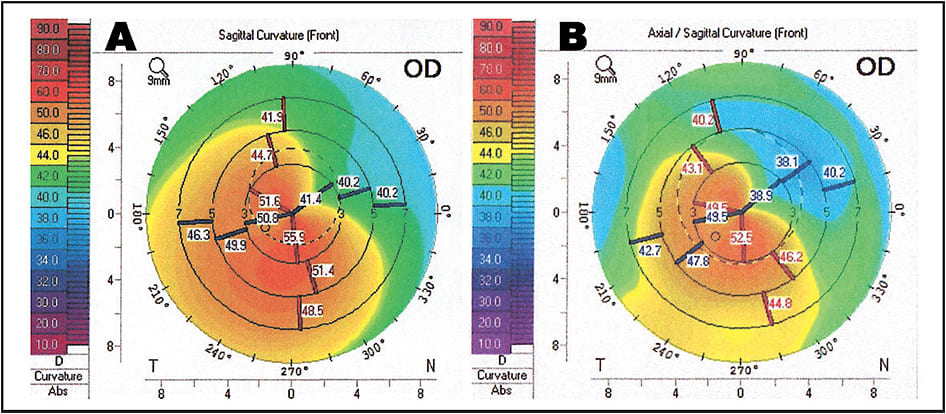
Figure 3. Axial curvature map OD of a patient who has keratoconus before ICRS implantation (A) and eight months after implantation (B).
Note the decrease in corneal irregularity after the procedure.
Using Both Procedures Together Although segment implantation flattens the central cornea, consequential shape changes in the periphery can pose obstacles in contact lens fitting. The challenge is created due to the increase in elevation above the segment and drastic depression adjacent to it. This change in elevation throughout the cornea will vary depending on the arc and width sizes used as well as the location and number of segments implanted. These irregularities in elevation may cause difficulties with centering a lens and may trap application bubbles in the areas of depression (Hladun and Harris, 2004; Uçakhan et al, 2006).
It is common to have both CXL and ICRS procedures performed on affected patients. Nevertheless, the combination treatment efficacy of these surgeries is still unclear. Several studies have reported that combined CXL and ICRS implantation—compared to each treatment alone—improved uncorrected and best-corrected acuity as well as keratometry readings (Saelens et al, 2011; Kiliç et al, 2012; Coskunseven et al, 2009). However, another study showed no difference in topographical and visual outcome in combined procedures (Cakir et al, 2013).
Contact Lens Fitting After Surgery
After surgery, it is important that the cornea is completely healed and topographic indices are stable before fitting a patient with contact lenses. Current literature states that corneal GP fitting can be initiated at three months (Louie et al, 2014; Tran and Edrington, 2007; McCandless, 2008). In my experience, a fitting can be completed as early as one month after CXL and/or ICRS implantation. Nonetheless, in most cases, three months is an ideal time to start contact lens fitting after each of these procedures.
With patients who have elected CXL and ICRS treatment, several factors should be met during the fitting process. First, the lens should provide adequate coverage of the cornea. Contact lenses, GP more so than soft, will center over the steepest part of the cornea. In post-ICRS implantation, the lens will decenter toward the peripheral segments. So, consider a larger-diameter lens to attain satisfactory corneal coverage.
Second, maintain a sufficient oxygen supply to the cornea to avoid hypoxic changes, including edema and neovascularization. To maximize oxygen transmissibility, it is important to prescribe lenses made from high-oxygen-permeable (high-Dk) materials.
Third, contact lenses should have a healthy mechanical fit with the ocular surface. In post-ICRS implantation, corneas will have an area of localized uneven elevation at the segment. It is important to confirm that the lens has a good mechanical fit and is not rubbing this area. Erosion of the overlying cornea may cause anterior displacement of the segment (Nosè et al, 1993).
Soft Contact Lenses In many cases, standard soft lenses can be fitted on patients in a conventional way and still provide adequate quality of vision. This is particularly true for patients who have mild ectasia and low power corrections. Any of the available daily or frequent replacement lens modalities are possible for fitting post-CXL or -ICRS implantation.
The material modulus and thickness will affect the way that a standard lens will fit. High-modulus (stiffer) lenses may result in fluting of the edges, while lower-modulus (softer) lenses may lay flat and drape over the entire cornea. Even with a low modulus, if the lens has an increased center thickness, this will create a stiffer profile and will make the lens more susceptible to fluting. For example, a high-powered soft lens that is thicker in the middle will tend to flute in comparison to a low-powered lens.
Nevertheless, traditional soft lens designs often provide less-than-optimal vision. In such cases, consider specialty soft contact lenses designed for irregular and surgically altered corneas. Specialty soft lenses provide sharper optics by having an increased center thickness to mask irregular astigmatism. Additionally, these lenses are available in higher sphere and cylindrical powers, and they have steeper central and peripheral curves to accommodate larger amounts of corneal irregularity.
Figures 4 and 5 show a patient who has post-LASIK ectasia and who underwent CXL in both eyes and ICRS implantation in the left eye. The patient is wearing a standard soft toric design in the right eye (Figure 4A) and a soft lens for irregular corneas in the left eye (Figure 5A). An optical coherence tomography (OCT) cross-section of each lens is shown for the right (Figure 4B) and left (Figure 5B) eyes; notice the thickness difference between the two designs.
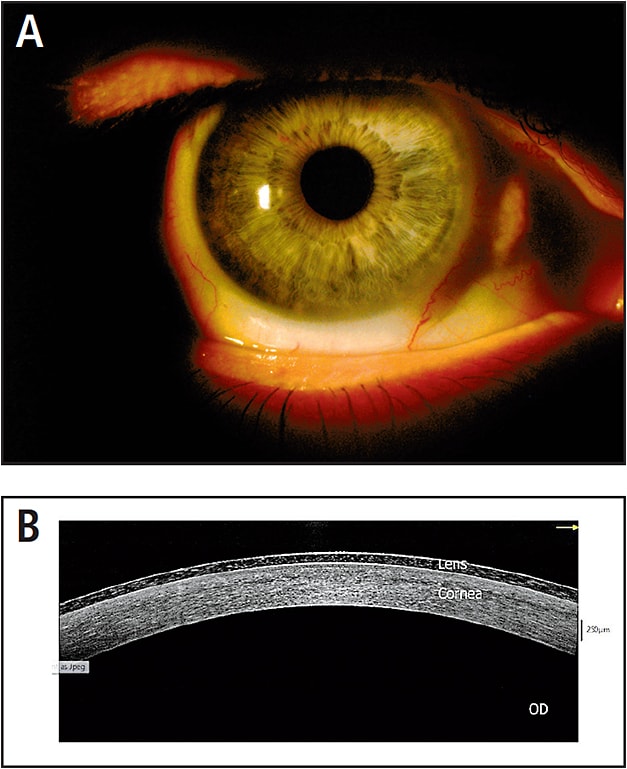
Figure 4. LASIK-induced iatrogenic corneal ectasia fitted with regular soft toric lens in the right eye (A). OCT cross-section over this lens (B).
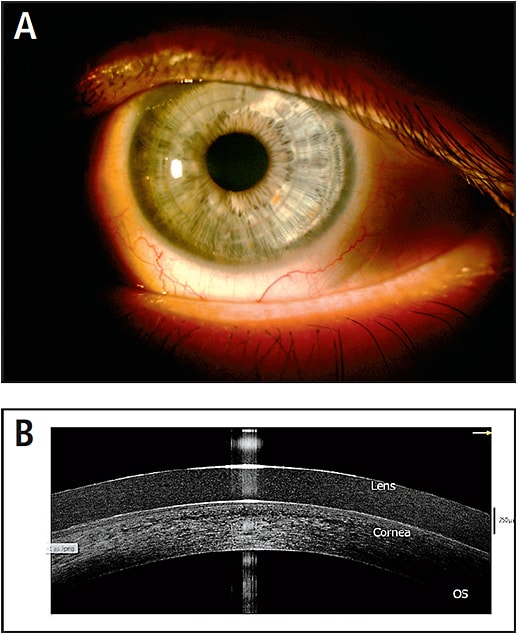
Figure 5. LASIK-induced iatrogenic corneal ectasia with ICRSs in the left eye fitted with specialty soft lens for irregular astigmatism (A). OCT cross-section over this lens (B). Note differences in lens thickness between the two lenses shown in Figures 4B and 5B.
Corneal GP Lenses Rigid contact lenses may be the only option to fully correct vision in ectatic patients who have undergone CXL and ICRS implantation. The differences in shape present between the surgically treated areas of the cornea and the areas that have not been altered make GP lenses challenging to fit. Often, corneal GPs do not exhibit a classic alignment pattern on a surgically altered cornea. Nonetheless, this may be acceptable as long as there is adequate lens movement, room for a healthy tear pump behind the lens, and the lens does not cause any harsh areas of punctate erosion.
Although there is mild corneal flattening after CXL, the overall corneal contour does not change dramatically. Thus, depending on the severity of the ectasia, you can fit corneal GP lenses in a conventional way. Keratoconus patients who have undergone CXL can be fitted into any of the available keratoconus lens designs.
In LASIK-induced iatrogenic corneal ectasia, the topography will have a combination of steeper areas at the site of the ectasia and in the untreated periphery, and it will be flatter in the non‐ectatic ablated areas. In post-LASIK ectatic patients who have undergone CXL, consider large-diameter lenses (i.e., greater than 10mm) for centration over the areas of ablation and ectasia (Steele and Davidson, 2007).
ICRS implantation creates a unique challenge in fitting corneal GP lenses due to the elevation over the segment and large areas of depression adjacent to it. Corneal insult over the segment from mechanical irritation must be avoided when fitting a corneal GP contact lens.
Larger-diameter corneal GP lenses center better over this broad area of irregularity and provide more sagittal depth to achieve light touch to vault over the segment. Figure 6 shows a patient in a large-diameter corneal GP that vaults over the ICRSs and centers adequately over the left eye.
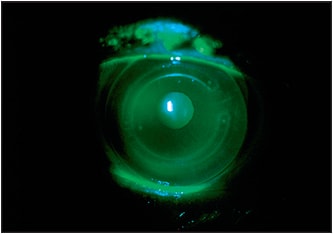
Figure 6. Large-diameter corneal GP fitted over ICRSs implanted for treatment of keratoconus in the left eye. Note the area of clearance over the ICRSs.
A reverse geometry design can also be used to fit patients post-ICRS implantation. In reverse geometry GP lenses, the peripheral curve adjacent to the optic zone is steeper in comparison to the optic zone radius.
A reverse geometry lens can be utilized after ICRS implantation if the back optic zone diameter approximates the size of the segment arc treatment zone (Louie et al, 2014) and the adjacent peripheral curve is wide and steep enough to either vault or align with the segment. The width of the optic zone created by ICRSs can range from 4.5mm to 7.0mm, and the segment width can range from 0.25mm to 0.45mm (Rabinowitz, 2010).
Piggyback Systems Many patients report corneal sensitivity over the segment after ICRS implantation. When fitting a corneal GP lens, a soft lens with a low power can be fitted underneath it to increase patient comfort. Additionally, the soft lens can aid in preventing mechanical irritation over the implanted ICRS. To minimize corneal hypoxia, fit a soft lens with a high Dk (Nosè et al, 1993; Louie et al, 2014; Smith and Carrell, 2008). Figure 7 illustrates a piggyback system over ICRSs in the left eye.
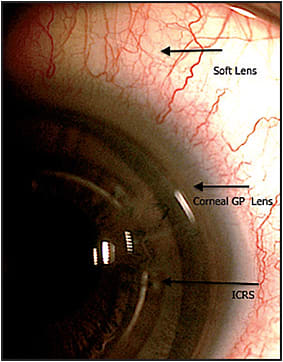
Figure 7. Soft lens piggyback system with corneal GP fitted over ICRSs for keratoconus in the left eye.
Hybrid Lenses Hybrid lenses may also be utilized in fitting those who have undergone CXL and ICRS procedures. Hybrids have a corneal GP center fused with a soft peripheral skirt. Newer hybrid lenses are made from high-Dk materials that allow assessment of fit using regular fluorescein.
Just as with corneal GP lenses, strive for an alignment fit with hybrid designs; however, this is typically very difficult to accomplish in ectatic and post-surgically altered corneas. Again, the lens fit is acceptable as long as it allows for healthy tear exchange and is not causing corneal irritation.
As a reminder, extra precaution must be taken over ICRS implants so as not to cause corneal erosion over the segments. This can be accomplished with a hybrid lens by making sure the GP center either aligns with, or vaults over, the ICRSs. Both regular and reverse geometry designs are available in hybrid lenses. Figure 8 shows a hybrid lens vaulting over ICRSs in the right eye.
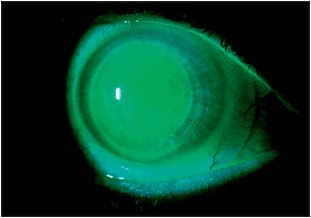
Figure 8. A hybrid lens vaulting over ICRSs in the right eye.
Scleral Lenses In contrast to fitting corneal GP lenses in which corneal topography is crucial to lens design, scleral lenses have the advantage of being able to vault the cornea and rest on the scleral‐conjunctival anatomy. This makes scleral lenses ideal for fitting over highly irregular corneas after CXL and ICRS.
These large lenses center well and offer stable vision and good comfort; additionally, their fluid‐filled reservoir offers therapeutic applications in the case of post-LASIK ectasia patients suffering from dry eyes (Parminder and Jacobs, 2015). Of additional benefit for patients who have ectatic disease, the large scleral lens diameter protects the cornea from eye rubbing and thus from inducing mechanical insult and potentially progressing their disease state.
Scleral lenses are available in both regular and reverse geometry designs. Figure 9 shows two patients who were successfully fitted with scleral lenses after ICRS implantation. The first patient had keratoconus and a pinguecula in the right eye, and so the periphery of the lens was notched (Figure 9A). The second patient developed dry eyes and ectasia after LASIK, and a scleral lens was used to rehabilitate his vision and treat the dry eye symptoms in his left eye (Figure 9B).
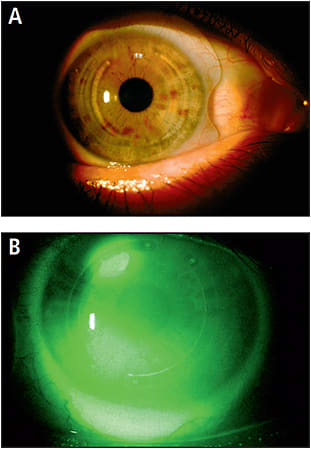
Figure 9. Scleral lens with notched peripheral haptic fitted over ICRSs for keratoconus in the right eye (A). Scleral lens fitted over left eye with LASIK-induced iatrogenic corneal ectasia implanted with ICRSs (B).
Summary
CXL and ICRS implantation are both commonly performed surgical treatment options for non-inflammatory corneal ectasias. Nonetheless, most patients who undergo these surgeries will still need to be fitted into a contact lens to reach their full visual potential. Knowledge of the various contact lens designs and the ability to interpret the corneal shape after CXL and ICRS implantation is key to helping this population succeed in contact lens wear. CLS
For references, please visit www.clspectrum.com/references and click on document #249.

| Dr. Frogozo specializes in adult and pediatric specialty contact lenses. She is the director of the Contact Lens Institute of San Antonio and the owner of Alamo Eye Care in San Antonio, Texas. She also is a consultant to CooperVision. You can contact her at contactlensinstitutesa@gmail.com. |