


Online Photo Diagnosis
BY LUCIANO BASTOS
Post-Intrastromal Ring Implant in a Case of Keratoconus
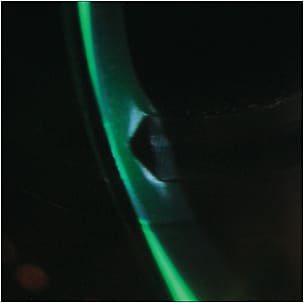
This image shows a close-up, cross-section view of a keratoconic cornea with an intrastromal ring. It clearly presents a triangular body in two semi-circular rings, which are utilized to exercise force from the center of the cornea to the periphery in an attempt to achieve a more stable corneal surface and neutralize most of the induced irregular astigmatism from the keratoconus.
Lens Fitting with Intrastromal Rings
A limited number of patients really benefit from this technique; claims that the procedure helps contact lens fitting1 are somewhat controversial. Some experienced surgeons claim that if the indication is correct and the correct intrastromal ring monogram is used, the results are better. However, these surgeons also acknowledge the unpredictability of the results. Each patient reacts differently, and only a limited number can really benefit from the procedure in terms of visual improvement outcomes.
When the visual outcome is not satisfactory, generally neither soft contact lenses nor spectacles alone will be sufficient to achieve visual rehabilitation. In most cases, the presence of intrastromal rings also makes GP fitting difficult due to the elevation created by the presence of the ring.2 Generally, this is more common at the inferior paracentral cornea.
This elevation can touch the posterior base curves of the GP lens, and the area becomes stressed by the lens movement. The result is corneal touch in a sensitive area in which the cornea is more rigid due to the presence of the implanted PMMA ring. Blinking will force the lid to push the lens against this area with every single blink, resulting in a permanent, light insult to the corneal epithelium—and eventually also to the stroma (corneal ulcer).
Even a piggyback technique usually fails when attempting to resolve these complex cases. This lens system also may bear against the implanted ring, and patients will only complain when there is a more extensive damage to corneal epithelium.
Under Pressure
Invariably, fitting a corneal GP in these cases results in epithelial abrasion. In this case, there was a significant amount of mechanical pressure at the inferior paracentral cornea where the temporal ring segment was located. Figures 2 and 3 show other views of the ring positions.
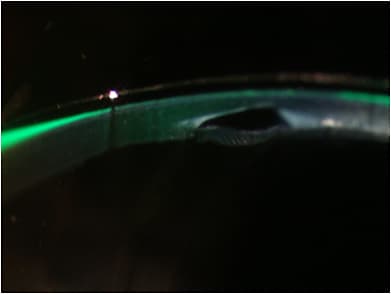
Figure 2. A closer view.
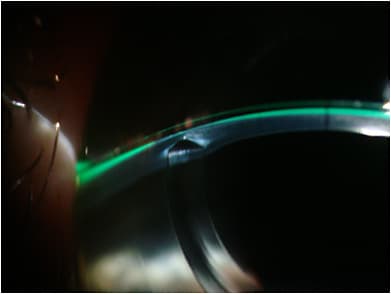
Figure 3. A wider view of the elevation created by the ring and its relation with the GP lens.
Our goal was to provide the patient with improved visual acuity and good comfort while also preserving corneal physiological health. Fitting a scleral lens to vault over the elevation caused by the intrastromal rings is usually the easiest way to manage such cases. In this case, it happened that the patient rejected the idea of fitting a scleral, mini-scleral, or even a corneo-scleral lens due to the lens size. Patients who have small palpebral fissures may also not be good candidates for these lens types.
Case Resolution
We ultimately fit a highly sophisticated, custom intralimbal GP design to overcome the inferior, paracentral elevation or at least to alleviate the pressure and allow tears to pass through that area (Figures 4 and 5). The lens has a diameter of 12mm and is manufactured in Optimum Extra material (100 Dk) (Contamac). The patient wears his lens for 12 to 14 hours daily without any complications. Figures 4 and 5 shows an excellent fluorescein pattern with an effective lacrimal pump and no compression to the area of the ring end where it created the anterior elevation.
Some cases may present microbubbles on lens application. Those bubbles form because we have to create a greater vault at the center and a better transition zone to overcome the inferior, paracentral, anterior elevation.
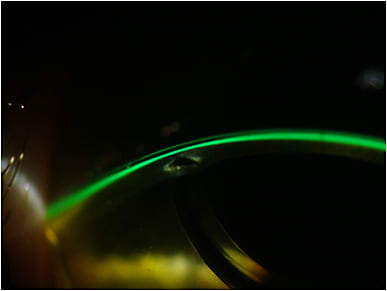
Figure 4. Intralimbal lens design that allowed us to resolve the case.
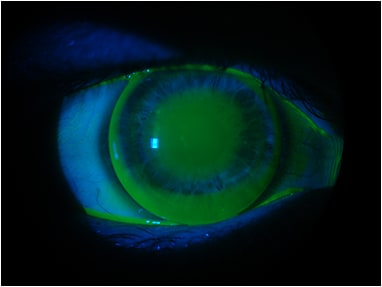
Figure 5. Frontal view fluorescein pattern.
Conclusion
Fitting post-intracorneal (intrastromal) ring patients with GPs is not an easy task. If a scleral lens is not an option, the best way to fit these patients is with larger GPs with an aspheric design that would vault the central cornea and slightly overcome the elevated area to avoid mechanical pressure and stress.
It is important to remember that patients who underwent ring implantation have likely already had bad results with the surgery itself and with successive failures in contact lens fitting experiences. They may feel like there is no hope for their case, especially if they saw a number of specialists before visiting your clinic. These patients must be well educated, and we cannot make promises but only try to find the best possible way to solve their challenge. They will be more cooperative if they are made aware of the complexity of their case and if you work with them to find a solution. It is also important to schedule frequent follow-up visits with these patients, especially during the first six months and then each year.
Luciano Bastos is the director and clinical instructor of specialty contact lenses at the Instituto de Olhos Dr. Saul Bastos (IOSB) and is the director and specialty lens consultant of Ultralentes, a small laboratory specializing in GP and scleral lens designs in Porto Alegre, RS, Brazil.