


SCLERAL PERIPHERAL CURVES
Beyond the Limbus: Scleral Peripheral Curves and Their Modifications
Whether to better fit an asymmetrical sclera or to accommodate a conjunctival anomaly, modifying peripheral curves can help improve fitting success.
By Stephanie L. Woo, OD, FAAO, FSLS, & Brooke Messer, OD, FAAO, FSLS
Scleral lenses are a great option for both irregular and regular corneas. The GP lens material and fluid reservoir create a functional optical system that negates both regular and irregular astigmatism. Scleral lenses give patients who have complex corneal conditions the best possible vision (Severinsky et al, 2014).
Scleral lens production has increased dramatically over the past few years, according to the Contact Lens Manufacturers Association. While scleral lenses are becoming a more popular option for practitioners and patients, it’s important to understand that fitting, evaluating, and managing scleral lens patients takes time, patience, and experience.
The scleral lens designs of today make it easy to achieve the basic needs for an acceptable fit, which includes a vault over the corneal apex of around 200 to 250 microns in depth. The vault should extend over the limbus area and land on the conjunctiva. The peripheral curves of the lens should bear the weight of the lens-tear layer system fairly evenly on the eye.
After working through a few scleral lens fittings, you might feel that scleral lenses are quite simple. Scleral lenses can be efficiently fit with some practice; however, it is the patient management and the lens troubleshooting that can lead to practitioner frustration. Most patients are satisfied with the vision that scleral lenses provide, but inadequate comfort and reduced cosmesis due to red eyes can lead to many lens remakes and adjustments.
Managing Blanching/Redness
One of the most common complaints that scleral lens fitters will hear from their patients is that they develop red eyes after wearing their lenses for a few hours or at the end of the day. Evaluating the pattern of any scleral vessel blanching on the eye can assist with your troubleshooting decisions.
Circumferential Blanching The most simple blanching pattern to observe and remedy is an evenly blanched conjunctiva 360º around the lens edge (Figure 1). In these cases, the problem is most likely that the edge of the scleral lens is too steep.
Figure 1. An example of 360º uniform edge blanching. Flattening the edge all around would help this patient.
A steep scleral lens edge will dig into the tissue near the edge and interfere with vascular blood flow. Dr. Christine Sindt uses the analogy of a high heel versus a snow shoe on soft ground to describe a steep edge fit. The high heel puts much pressure on a very small area of the conjunctiva. This will pinch the conjunctiva, cutting off the vessel flow in the area and leaving it blanched. A remedy to this type of blanching is a flatter edge curve, which will act more like a snowshoe than a high heel. A flatter edge will distribute the lens weight more evenly and thus reduce conjunctival blanching.
When the design allows, another adjustment that would further reduce vessel blanching from a tight edge is extending the length of the landing curves, which provides a larger area on which to distribute the lens weight.
Asymmetric Blanching Another conjunctival blanching pattern observed in scleral lens wearers is asymmetric or non-uniform blanching (Figure 2). In these cases, the area of excessive blanching or bearing is usually perpendicular to areas of edge lift or alignment due to the anatomical shape of the eye.

Figure 2. An example of non-uniform scleral lens edge blanching, typically at 3 o’clock and 9 o’clock. This patient would benefit from a toric haptic system.
The Pacific Scleral Lens Study measured 96 eyes and 1,536 scleral angles to assess anatomical shapes of normal and keratoconic eyes (Kojima et al, 2013). A chord length was set to 15.0mm and also to 20.0mm (Figure 3). At the 15.0mm chord, the variability among the scleral angles measured in eight different quadrants ranged from 37.6º to 39.3º (Figure 4). At the 20mm chord, the variability increased, ranging from 36.6º to 43.2º (Figure 5). This indicates that the further away from the limbus, the greater the variability in scleral shape. What this means is that the need for toric peripheral curves with scleral lenses will increase as the lens diameter increases.
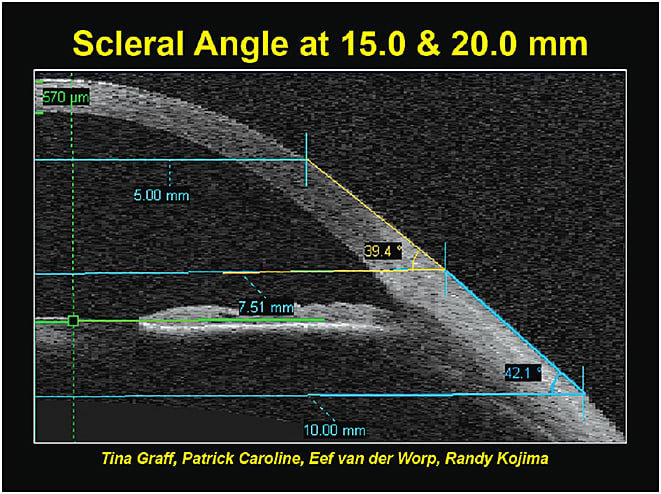
Figure 3. The Pacific Scleral Lens Study measured the scleral angles at chords of 15mm and 20mm.
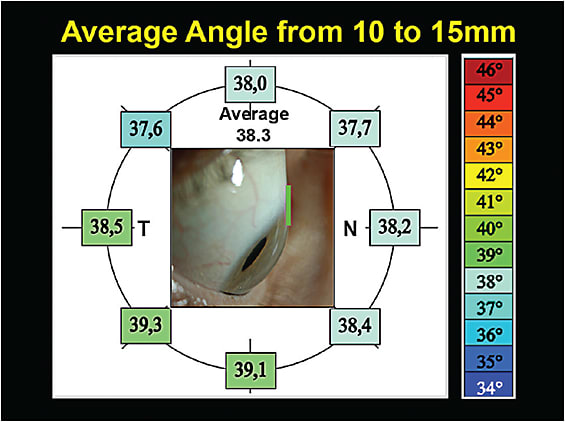
Figure 4. The average scleral angle at a chord of 15mm showed very little variation in eight quadrants of the eye.
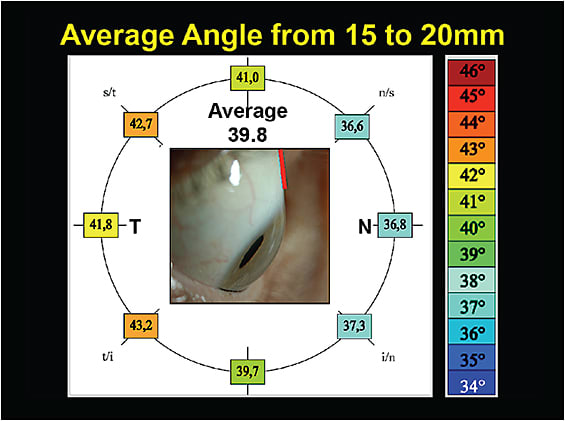
Figure 5. The average scleral angle at a chord of 20mm showed much more variation, indicating that the sclera becomes more asymmetric further away from the limbus.
Dr. Greg DeNaeyer states: “Some patients have asymmetric scleral anatomy that results in a poor fitting relationship when fit with a scleral lens that has a spherical haptic surface. These poorly fitting lenses often exhibit a with-the-rule appearance. The lens will have 3 o’clock and 9 o’clock compressions, as well as excessive lift at the 6 o’clock and 12 o’clock positions.
“In these instances, some manufacturers offer toric back surface haptic (peripheral curves), which can dramatically improve the scleral lenses’ fitting relationship,” (DeNaeyer, 2012). According to Dr. DeNaeyer’s most recent analysis, about 85% of his 16mm diameter scleral lenses utilize back-surface toric haptics (most being with-the-rule).
When designing a lens with toric peripheral curves, you need to communicate the amount of toricity desired to the laboratory. Each scleral lens has a different design system, some requiring amounts in diopters of toricity, while others require “steps” of toricity or microns of lift in one meridian.
Fitting and Troubleshooting Tips
Dr. Woo’s tips:
• If you fit smaller-diameter lenses, the need for a toric periphery is rare. In my clinic, 90% of all scleral lens fits are 15.0mm in diameter or smaller. Out of all of my scleral lens fits, only about 15% require a toric peripheral curve.
• When you see blanching at 3 o’clock and 9 o’clock, this is a good indicator that a toric peripheral curve may help.
• The edges may look aligned during lens fitting and dispensing, but the real indicator will be when patients arrive for the follow-up visit (preferably in the afternoon, after they have worn the lenses for a few hours). This is due to the natural lens settling that occurs over hours of scleral lens wear. The lens will settle onto the flatter meridians of the sclera (usually 3 o’clock and 9 o’clock) and cause these areas to become compressed, while leaving the steeper areas well aligned (or, in extreme cases, with edge lift).
• True scleral lens fitting experience is gained when you see patients month after month and year after year. The evaluation of the lenses and ocular health, along with the feedback that you obtain from patients, is extremely valuable at these intervals.
Dr. Messer’s tips:
• When selecting a scleral lens design, corneal diameter is king. If the corneal diameter is large, the lens diameter also needs to be large enough to ensure adequate limbal clearance. More than half of the scleral lenses fit in my clinic are larger than 16.0mm in diameter and have toric peripheral curves.
• Adding toric peripheral curves to a scleral lens can have an added bonus by reducing chamber clouding in many patients. When a patient notes chamber clouding, apply fluorescein over a settled scleral lens and observe whether the fluorescein works its way into the post-lens tear layer. If you see fluorescein in the chamber after a few minutes, adding toric peripheral curves can reduce chamber debris by limiting tear exchange.
• Toric peripheral curves on scleral lenses can improve vision, too. Improving the alignment of the lens to the sclera reduces the incidence of lens flexure. Prior to the availability of toric peripheral curves, the only way to combat flexure was to decrease lens diameter or increase lens thickness. A toric haptic system allows you to use the desired lens diameter without increasing lens thickness, which maintains oxygen permeability as a result.
• When patients note reduced wearing time due to lens discomfort, toric peripheral curves can be a great tool. A study by Visser et al (2006) found that patients using scleral lenses were able to wear their lenses two more hours each day after toric peripheral curves were added.
When observing a fit with mild-to-moderate blanching in the horizontal meridian and no blanching in the vertical meridian, a toric peripheral curve described as 3 diopters, 2 steps, or 60 microns of lift would likely be appropriate. If edge lift is observed on the vertical meridian and excessive blanching in the horizontal meridian, an adjusted toric lens with 5 diopters, 4 steps, or more than 100 microns of lift in toricity would be a good starting point in ordering a new lens.
Anterior segment photos documenting the amount of vessel blanching can be very helpful in achieving an accurate scleral lens design; a laboratory consultant can review the photos and assist in determining the amount of toricity needed in the haptics of the adjusted scleral lens.
Conjunctival Anomalies A final thought on scleral lenses and their peripheral curve adjustments is to evaluate for conjunctival anomalies, such as pingueculae and cysts. Due to their elevated anatomy, pingueculae and cysts would result in excessive conjunctival blanching in a focal area. Toric peripheral curves can reduce the bearing on these areas, but many times a notch or microvault is needed to significantly reduce the compression over these elevations.
Improve Your Scleral Fitting Success
While fitting scleral lenses requires different considerations compared to fitting soft lenses or corneal GP lenses, it becomes easier once you understand the mechanics of the lenses and the shape of the eye. With many patients having asymmetrical scleras or conjunctival anomalies to accommodate, knowing how to modify the peripheral curves of scleral lenses can really boost your success rates. For more tips on scleral lens peripheral curve fitting and troubleshooting, see the sidebar on p. 32. CLS
For references, please visit www.clspectrum.com/references and click on document #243.

| Dr. Woo currently practices at Havasu Eye Center in Lake Havasu, Ariz. She is also the public education chair for the Scleral Lens Education Society and is an Advisory Board member for the GPLI. She is a consultant to Blanchard, X-Cel, and SpecialEyes. |

| Dr. Messer practices in Minneapolis in a private optometry office focused on specialty contact lenses. She is a consultant to Precilens, has received research funding from B+L, and has received honoraria from the STAPLE program and Alden Optical. |