


The Scleral Lens Vault
Scleral Lenses for Exposure Keratopathy
BY GREGORY W. DENAEYER, OD, FAAO

The anterior ocular surface requires continuous hydration from tears to prevent desiccation of its non-keratinized cellular tissue. Lack of a continuous fluid layer may lead to the destruction and loss of corneal epithelial cells, resulting in patient discomfort and vision loss. The lacrimal system, lids, and associated glands are responsible for producing and maintaining a hydrated surface.
Nerve damage or direct trauma can lead to loss of lid function that results in exposure and desiccation. Facial nerve palsy causes loss of function of the orbicularis oculi, which is responsible for lid closure. Facial nerve palsy can occur secondary to Bell’s palsy, trauma, infection, neoplasms, and congenital anomalies (Alsuhaibani, 2010). Patients who are sedated during hospital stays are also at risk for incomplete lid closure that results in exposure. The incidence of exposure keratopathy for a two- to seven-day stay in the intensive care unit ranges from 20% to 42% (Shan and Min, 2010).
The Impact of Exposure
Acute and chronic exposure that leads to exposure keratopathy will cause discomfort. Chronic exposure keratopathy can lead to corneal thinning, scar tissue, and irregularity that can reduce a patient’s best-corrected vision with glasses or soft lenses (Figure 1). Traditional management includes artificial tears, lubricating ointments, bandage soft lenses, tarsorrhaphy, and eyelid weights. However, scleral lenses can be prescribed for acute or chronic exposure keratopathy (Figure 2). Scleral lenses offer protection and a continuous fluid interface despite a patient’s inability to obtain full or complete eyelid closure.
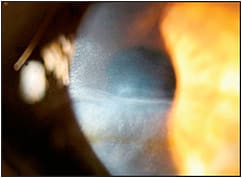
Figure 1. Corneal thinning and scarring secondary to chronic exposure after a hospital stay for Guillain-Barré.

Figure 2. Scleral contact lens fit on a patient who has lagophthalmos.
Weyns et al (2013) reported on a study of three patients who were fit with scleral lenses after developing unilateral lagophthalmos and corneal anesthesia post tumor resection. Two patients were unhappy with previous tarsorrhaphy secondary to visual restriction, and a third found tarsorrhaphy cosmetically unacceptable. The patients were successful with scleral lenses with a minimum wear time of 10 hours per day. The authors concluded that, for cases of exposure, scleral lenses could successfully protect the surface in a cosmetically acceptable way while optimizing vision.
Another case reported by Grey et al (2012) demonstrated successful scleral lens management of a patient who had bilateral palsies of cranial nerves V, VI, and VII after previous standard treatments, including bandage soft contact lenses, had failed to improve visual acuity.
Conclusion
In my opinion, scleral lenses are perhaps the best option for exposure keratopathy. They can improve comfort and vision without the need for tarsorrhaphy. CLS
For references, please visit www.clspectrum.com/references and click on document #248.
Dr. DeNaeyer is the clinical director for Arena Eye Surgeons in Columbus, Ohio and a consultant to Visionary Optics, Alcon, B+L, and Aciont. He is also a shareholder in Precision Ocular Metrology LLC. You can contact him at gdenaeyer@arenaeyesurgeons.com.