


SCLERALS FOR OSD
Utilization of Scleral Lenses for Ocular Surface Disease
Scleral lenses can protect, lubricate, and support the ocular surface.
By Melissa Barnett, OD, FAAO, FSLS
Dry eye is a highly prevalent condition, ranging from approximately 7% to 34% of patients depending on geographic location (Lin et al, 2003; McCarty et al, 1998). In the United States, an estimated 23 million people age 20 years and older report dry eye disease of any severity (Market Scope, 2004). In clinical practice, we observe that patients who have clinical signs and symptoms of dry eye disease are more likely to experience contact lens discomfort (Begley et al, 2001).
With age, dry eye is even more prevalent, which may exacerbate contact lens discomfort. Dry eye has many presentations and can range from mild to moderate to severe. Dry eye symptoms include feelings of dryness, pain, stinging, and/or burning; itchy eyes; sandy, gritty, or foreign body sensation; photophobia; excessive tearing; and blurry or interrupted vision.
An example of mild dry eye may be a patient who has refractive error and high visual needs, including smart phone and computer use. A moderate dry eye patient may be a patient who has exposure keratitis, Sjögren’s syndrome, or Salzmann’s nodular degeneration (Figure 1). Examples of severe dry eye include graft-versus-host disease (GVHD), Stevens-Johnson syndrome, or limbal stem cell deficiencies. In all forms of dry eye, but especially in the severe ocular surface disease population, scleral lenses are an option to alleviate symptoms of dry eye that may be debilitating (Figure 2).

Figure 1. Scleral lens on a patient who has Salzmann’s nodular degeneration.
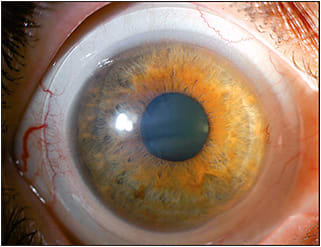
Figure 2. Scleral lens on a patient who has dry eye.
Scleral lenses are advantageous to protect, lubricate, diminish pain, reduce ocular symptoms, and support the ocular surface. In advanced dry eye cases, visual rehabilitation may not be the goal. In some instances, improvement of vision is obtainable, but not always.
In clinical practice, it is helpful to document the goal of scleral lens therapy and to continuously educate our patients regarding visual expectations. Scleral lenses may also not eliminate the need for adjunctive therapy, such as artificial tears, topical cyclosporine 0.05%, topical steroids, autologous serum, or punctal plugs. Educating our patients, their families, and our staff of the need for adjunctive therapy has been beneficial in my practice.
Evaluating Ocular Surface Disease
Examining the ocular surface is critical in all patients. There are numerous testing modalities that allow practitioners to evaluate their patients. This article will highlight some of these, but it is not a comprehensive review.
Ocular Staining Ocular staining is evaluated with sodium fluorescein, rose bengal, and lissamine green. Fluorescein stains defects in the corneal and conjunctival epithelium, among other things. A wet fluorescein strip is applied to the conjunctiva to evaluate staining of the conjunctiva and cornea.
Rose bengal is used to stain dead conjunctival cells or cells unprotected by the normal mucin layer. Rose bengal stains the conjunctiva more than it stains the cornea. This correlates well with the degree of aqueous tear deficiency, tear breakup time (TBUT), and reduced mucus production by conjunctival goblet cell and non-goblet epithelial cells. Rose bengal is available in strips or as 5mL bottles of 1% rose bengal. The downside of rose bengal is that it may irritate, and be toxic to, the ocular surface.
Lissamine green has a similar mechanism of staining as rose bengal does; however, it is less irritating. A wet lissamine green strip is applied to the conjunctiva to evaluate staining.
Tear Production A Schirmer’s test is used to evaluate aqueous tear production with a special filter paper (no. 41 Whatman) that is 5mm wide and 35mm long. Schirmer 1 is performed without anesthetic, and Schirmer 2 is performed with anesthetic. In theory, both Schirmer 1 and 2 evaluate baseline secretion; Schirmer 2 also measures reflex secretion. A Schirmer’s strip is placed under the lower lid. After five minutes, the strip is removed and the results are analyzed. More than 10mm of moisture on the filter paper after five minutes is considered normal.
Another method to evaluate tear production is the Phenol red cotton thread test. This test takes 15 seconds per eye, and no anesthetic is needed. The color change in the cotton thread can be confirmed hours after testing.
Another test of aqueous tear production is the fluorescein clearance test. This test may be more accurate; however, it is rarely performed in clinical practice. The fluorescein clearance test measures the clearance of 5mL of 2% sodium fluorescein that has been instilled into the eye. Then, after 15 minutes, the color of the lateral tear meniscus is evaluated using fluorophotometry and is matched to a scale. Dry eye causes delayed clearance of fluorescein. The rate of clearance relates to tear production. A value of three is the threshold between normal patients and symptomatic patients.
Matrix Metalloproteinase-9 (MMP-9) Detection InflammaDry (Rapid Pathogen Screening, Inc.) is a test that is similar to an at-home pregnancy test (Chotikavanich et al, 2009). InflammaDry takes a sample of a patient’s tears and gives a positive (ocular surface disease) or negative (no ocular surface disease) result in 10 minutes. During the test, a red line indicates elevated MMP-9, with a stronger red line indicating more significant ocular surface disease. The test is based on a quantifiable value of the amount of MMP-9 in the tears. More than 40ng/mL of MMP-9 indicates a positive InflammaDry test.
MMP-9 is a proteolytic enzyme secreted from stressed epithelial cells on the ocular surface and is a non-specific marker of inflammation. The InflammaDry test does correlate with dry eye, ocular surface disease, and some clinical findings. More positive results are associated in both Sjögren’s syndrome and meibomian gland dysfunction.
Impression Cytology Impression cytology is a method of collecting conjunctival epithelial cells for analysis of ocular surface disorders. A cytology membrane is pressed against the conjunctival surface, removed, and then stained with Periodic Acid-Shiff stain or antibodies.
The analysis includes shape, number, density, and pathologic modifications of epithelial cells, goblet cells, and inflammatory cells. Although impression cytology provides information about ocular surface disease, it is not practical for clinical practice.
Tear Osmolarity Tear osmolarity is important for many aspects of epithelial and nerve cell function. In healthy tears, the electrolyte concentrations are maintained to ensure correct osmolarity. However, in unhealthy tears, proteases are activated, which degrade the extracellular matrix and the tight junctions between adjacent cells of the corneal epithelium. Activated proteases are responsible for cleavage of cytokines into an activated pro‐inflammatory form. A subsequent increase in electrolyte concentration increases tear osmolarity. Elevated osmolarity can cause less regulation of the tear film, more damage to the ocular surface, and more inflammation. Increased rates of tear evaporation lead to a more concentrated tear film (increased osmolarity). Increased tear evaporation is present with both aqueous deficient and evaporative dry eye disease.
The TearLab Osmolarity System (TearLab Corporation) measures the osmolarity of the tears and, according to the company, is a sensitive marker for dry eye. The TearLab Osmolarity Test Card determines tear osmolarity using nanoliter volumes of tear fluid collected directly from the eyelid margin. Specifically, a 50nL sample of tears is taken in vitro for diagnostic use.
The system utilizes a temperature-corrected impedance measurement to provide an indirect assessment of osmolarity. After applying a lot-specific calibration curve, osmolarity is calculated and displayed as a quantitative numerical value. Osmolarity values above 308mOsms/L are generally indicative of dry eye disease.
Corneal Topography The Oculus Keratograph Topography System (Oculus Corporation) can perform a non-invasive assessment of tear meniscus height. Tear meniscus height is an indicator of ocular surface tear volume. Topography measures the inferior tear meniscus height via imaging of the anterior ocular surface. It projects a small horizontal light that reflects off of the top of the tear meniscus and is able to directly measure the height of the inferior tear meniscus in millimeters.
The computer analyzes the reflected Placido ring mires and measures the breakup time throughout the surface measured. Time measures of localized tear breakup are recorded to the 0.10 of a second. Breakup times of greater than 14 seconds are considered normal. Between 13 and 8 seconds are considered borderline. Seven seconds and below are considered abnormal.
History of Scleral Lenses for Ocular Surface Disease
There has been an extensive, well-reported history of scleral lens use for patients suffering from ocular surface disease. Scleral lenses were first described in medical literature back in the late 1800s (Bowden, 2009). Around 1888, Adolf Fick described blown glass “vesicles,” and Eugène Kalt used a glass “contact shell” to improve vision in keratoconus patients. August Müeller expressed interest to correct his high myopia (around –14.00D) with ground glass lenses in 1889. Additionally, F. Ad. Müller Söhne developed a scleral shell around 1887.
Although the lenses did improve vision, the manufacturing process at that time was challenging, and the lenses were difficult to reproduce. In addition, wearing the lenses quickly caused symptoms of oxygen deprivation. Therefore, scleral lenses were not widely used.
In the early 1900s, the development of polymethylmethacrylate (PMMA) made it somewhat easier to manufacture lenses. Because PMMA is moldable, the lens could be made using an impression mold of the ocular surface. However, the manufacturing process remained cumbersome, and it was virtually impossible to reliably reproduce lenses. In addition, PMMA material is not oxygen-permeable.
In 1943, Klein reported two cases of neuroparalytic keratitis in the British Journal of Ophthalmology. In 1962, Ridley did an extensive review of 3,000 cases using scleral lenses as therapeutic treatment. And, Gould reported the treatment of neurotrophic keratitis with scleral lenses in 1967.
In 1983, Ezekiel published that “Ocular conditions that are especially suited for haptic lenses include...Corneas which are disrupted, distorted, or dry due to lid deformities....” Subsequent articles were then released in the 1990s by authors including Schein et al (1990), Kok and Visser (1992), and Pullum and Buckley (1997).
What Does the Recent Literature Say?
General Benefits of Sclerals Bavinger et al (2015) recently published an evidence-based review of scleral lens use in dry eye syndrome. The authors reported that scleral lenses are a viable option for severe dry eye and that they were both well tolerated and effective. Benefits included improved visual acuity and relief of symptoms.
Of particular interest, the authors reported that there are currently 18 manufacturers of scleral lenses—but there may be even more. The authors suggest that further research is needed to standardize outcome measures and to compare different sizes and types of lenses.
GVHD GVHD occurs in patients who have undergone allogenic hematological stem cell transplantation. It also may occur in either acute or chronic forms, although the chronic form is more common. Ocular signs and symptoms are present in 40% to 90% of patients who have chronic GVHD.
Ocular GVHD is a T-cell mediated process that occurs when donor lymphocytes attack host histocompatibility antigens. This inflammatory process leads to inflammation of the lacrimal gland, conjunctiva, and ocular surface, which eventually causes a decrease in the density of conjunctival goblet cells and scarring of the lacrimal gland and conjunctiva. Decreased tear production is a result of lacrimal gland scarring.
There are multiple symptoms of ocular GVHD, which can include dry eye, foreign body sensation, redness, irritation, epiphora, photophobia, blurred vision, and severe pain. Ocular findings can range from moderate-to-severe keratoconjunctivitis sicca, bilateral marginal keratitis, filamentary keratitis, anterior uveitis, corneal ulceration, or neovascularization. A pseudomembrane or membrane may be present. In severe ocular GVHD, corneal erosions, corneal thinning, ulcerations, and possible perforations may be present.
Treatments can include topical nonpreserved artificial tears, topical cyclosporine 0.05%, tacrolimus and autologous serum. As indicated by Malta et al (2010), cyclosporine A is a T-cell inhibitor that helps to down-regulate inflammatory cytokines in the conjunctiva.
Keratoconjunctivitis Sicca An article published by Rossi et al (2015) evaluated scleral lenses for the management of severe keratoconjunctivitis sicca secondary to chronic GVHD. A retrospective study of 16 patients was performed from June 2009 to November 2013. Patients were fit with scleral lenses for severe keratoconjunctivitis sicca associated with chronic GVHD. Best-corrected visual acuity and quality of life measured by the Ocular Surface Disease Index (OSDI) and National Eye Institute Visual Function Questionnaire-25 (NEI-VFQ-25) were assessed. These outcomes were evaluated prior to scleral lens fitting and six months after scleral lens wear.
All 16 patients reported improvement of their ocular symptoms. Best-corrected visual acuity, OSDI, and NEI-VFQ-25 improved six months after scleral lens fitting. There were not any serious adverse events, infections, or hypoxic or allergic complications attributable to scleral lenses. The authors reported that scleral lenses appear to be safe and effective in patients who have severe dry eye related to chronic GVHD.
Dry Eye Due to Keratoconus Many of our patients who have keratoconus also experience dry eye on a regular basis. A study published by Carracedo et al (2016) looked at patients who have keratoconus and evaluated the effect of scleral lenses on dry eye biomarkers. Twenty-six keratoconus patients (with or without intrastromal corneal rings) were included in the study. OSDI, Schirmer’s test without anesthesia, TBUT, MMP-9 concentration, osmolarity, and diadenosine tetraphosphate (Ap4A) concentration were examined before and after wearing a scleral lens for eight hours.
Ap4A is an intracellular signal molecule that is produced due to adverse environmental factors. Ap4A is released from the corneal epithelium, stimulating tear production, and is a physiological modulator of tear secretion (Peral et al, 2006). In patients who have dry eye, Ap4A may be up to five times higher than in patients who have a normal lacrimal functional unit (Peral et al, 2006). In dry eye patients who have reduced tear production, Ap4A may be 100 times higher (Peral et al, 2006).
The mean scleral lens sagittal depth ranged from 4,200μm to 4,800μm. There were no significant changes in Schirmer’s test and TBUT in either group. OSDI and osmolarity were lower after wearing scleral lenses in both groups. Ap4A concentration was lower after scleral lens wear in the keratoconus group but not in the intrastromal corneal ring group. MMP-9 concentration was elevated after wearing scleral lenses in both groups. The authors suggest that scleral lens wear improves the symptoms and some clinical signs of dry eye. The authors propose that the increase of MMP-9 concentration could be caused by tear film stagnation and use of preserved saline.
Debris and How to Remove It
While there is significant evidence that scleral lenses are helpful for dry eye, there are also some complications when fitting patients with scleral lenses for dry eye. Debris is the most common problem with scleral lens wear and severe dry eye. It is important to inform patients of this issue prior to scleral lens fitting.
The front surface of a scleral lens may be polished; however, this will also polish off the plasma surface. Adding a plasma treatment or reapplying it is an option. With a plasma surface treatment, hydrophobic elements are removed from the surface of a lens through electrostatic discharge.
Plasma treatments to the surface are used to remove any remaining residue from the lens after the manufacturing process, increase comfort and decrease lens awareness by creating a very clean lens, maximize wettability of the lens, provide possible resistance of protein and bacterial deposits, and create crisp vision through the lens. Avoid plasma treatments on crazed lenses.
It is helpful to ask patients about what type of hand soap is used. If necessary, advise patients to change their soap to a contact lens or acne treatment hand soap to avoid surface debris.
Makeup can also contaminate the front surface of the lens, causing cloudy vision and decreasing the lens wettability. Contamination occurs because a scleral lens is two to five times thicker compared to other lens designs and can protrude from the front surface of the eye due to the amount of apical clearance under the lens. Instruct patients to remove the lens, clean, and reapply it if makeup adheres to the front surface of the lens. It is recommended to apply creams and makeup after scleral lens application.
To eliminate non-wetting or deposits, it is beneficial to polish lenses with a laboratory cleaner or an alcohol-based daily cleaner, then rinse and rub the surface with a soft multipurpose contact lens solution. Additionally, laboratory cleaners used in-office remove pitch, wax, and other solvents used in the manufacturing process in addition to lipids, body oils, and other contaminants.
In my experience, switching to a peroxide-based disinfection solution is also helpful to eradicate surface deposits. Also available is a two-component cleaner with sodium hypochlorite and potassium bromide that can remove deposits, bacteria, fungus, molds, and yeasts.
On-eye surface cleaning using a saline-moistened cotton swab or eye shadow applicator, or a wet scleral lens applicator, can remove surface debris. In addition, increased lubrication over the lens throughout the day may be beneficial.
Avoiding debris may require aggressive treatment and management of the eyelids, including treatment of meibomian gland dysfunction, with mechanical, topical, and oral methods, which have all proven to be beneficial. Recommending dietary changes, such as taking Omega-3 supplements and reducing fried and fatty food, can be helpful as well.
Front-surface debris and chamber debris are managed differently. Reservoir debris can cause cloudy vision. To manage reservoir debris, patients should remove, clean (if needed), and reapply the scleral lens as needed. Lens modifications including decreasing the central vault, reducing the diameter, and incorporating a toric-back-surface design may help to reduce reservoir debris. A more viscous solution with lens application is also beneficial to reduce reservoir debris. When in doubt, always re-evaluate the care and handling of scleral lenses.
Conclusion
In the past, dry eye was often the downfall of patients desiring, or in need of, contact lenses. In 2016, scleral lenses provide enhanced ocular health, comfort, and vision to patients plagued by ocular surface disease. And, scleral lenses have given many patients an unparalleled quality of life compared to their pre-scleral life. CLS
For references, please visit www.clspectrum.com/references and click on document #248.

| Dr. Barnett is the principal optometrist at the UC Davis Eye Center in Sacramento, CA. She is a Fellow of the American Academy of Optometry, a Diplomate of the American Board of Certification in Medical Optometry, and she serves on the Board of Women of Vision, Gas Permeable Lens Institute, Ocular Surface Society of Optometry, and The Scleral Lens Education Society (SLS). She is an advisor to AccuLens, Alcon, Alden Optical, Allergan, CooperVision, Bausch + Lomb (B+L), Novabay, Johnson & Johnson Vision Care, and the SLS, and she has received honoraria and/or travel expenses from Alcon, AccuLens, Alden Optical, Allergan, B+L, Johnson & Johnson Vision Care, and SLS. |