


ORTHOKERATOLOGY
Fitting Ortho-K Lenses Post-PRK or Post-LASIK
The when and how of orthokeratology after refractive surgery.
By Randy Kojima, FAAO, FBCLA, FSLS, FIAO, & Cindy Ho, BSc, OD, PhD
Orthokeratology treatment creates a temporary and reversible reduction in myopia for patients of virtually any age (Nichols et al, 2000; Tahhan et al, 2003; Walline et al, 2009). However, orthokeratology is primarily fit on adolescents as a myopia control device in many countries around the world (Cho et al, 2005; Kakita et al, 2011; Hiraoka et al, 2012; Santodomingo-Rubido et al, 2012).
Annual polls taken at the Vision by Design meeting in the United States suggest that less than 10% of orthokeratology treatments are performed on adults. Although they represent the smaller component of fits, these patients are usually highly motivated to achieve the freedom from glasses and contact lenses during the day that orthokeratology provides.
Similarly, many more adults have chosen refractive surgery for the same reason, but a percentage may be left with residual prescriptions at some point following the procedure (O’Doherty et al, 2006; Zalentein et al, 2009; Alió et al, 2015). Inadequate corneal thickness may prohibit enhancement for some patients; for others, additional surgery may be undesirable (Randleman et al, 2009; Vaddavalli et al, 2013). These are interested candidates who chose freedom from correction to begin with and who continue to be interested in life without daytime glasses or contact lenses. Could orthokeratology offer these patients an alternative to glasses, contact lenses, or additional surgery?
The real contact lens fitting challenge following surgical myopia reduction is the change in corneal curvature from a prolate to a more oblate shape (Yu, 2009; DeNaeyer, 2011). This alteration increases the complexity of the fit and may greatly impact our goals of attaining proper centration, alignment, comfort, and desired myopia reduction.
In the prolate, non-surgical eye, orthokeratology can be a very predictive and relatively straightforward procedure (Tahhan et al, 2003). In the post-surgical eye, it can ultimately represent a significant amount of chair time and can accrue expenses with the laboratory that appear to have no end in sight. Therefore, we have to consider: when are the conditions right to fit a postphotorefractive keratectomy (PRK) or post-laser-assisted in-situ keratomileusis (LASIK) patient, and how do we achieve a successful outcome?
Patient Selection
First and foremost, you must ensure that you have selected a good candidate for this procedure. Patients should have an uncomplicated surgical history and show no clinical signs of being at risk during overnight contact lens wear.
Slit lamp assessment should confirm good corneal health and integrity, while the topography should be devoid of irregularities beyond that which would be expected following refractive surgery. You should also ensure that the best-corrected visual acuity (BCVA) is 20/20.
In addition to the careful monitoring of eye health necessary with every orthokeratology fit, special care and consideration must be taken with post-LASIK patients to monitor for any changes in the corneal flap and interface. Keep in mind that a standard LASIK flap has a thickness of approximately 170 microns (Yan et al, 2007) and that orthokeratology treatment involves only the superficial, approximately 10 microns of corneal tissue (Alharbi and Swarbrick, 2003).
GP fitting can be safely performed six to 12 months after refractive surgery. As a general guideline, wait a minimum of one year after surgery before fitting orthokeratology lenses; the corneal topography and refraction should be stable for at least six months (Astin et al, 1996; Horn, 2002; Williams, 2006).
A Representative Clinical Case
Patient X underwent bilateral LASIK to correct a moderate degree of myopia. Approximately five years after the initial procedure, he began to experience some myopia regression. Ten years after his LASIK treatment, he presented to the office with a refraction in the right eye of –1.50 –0.75 x 180 and in the left eye of –1.75. He had no record of his pre-operative refraction or keratometry readings but recalled an Rx of approximately –6.00D in both eyes.
Corneal pachymetry readings were approximately 470µm bilaterally. The corneal topographies revealed normal post-LASIK curvature with no evidence of corneal ectasia and subtle superior decentration of the LASIK ablation in both eyes (Figure 1). The corneal health was excellent with BCVA of 20/20 in each eye, but his chief complaint was blurry vision throughout the day that seemed to be gradually worsening over the years.
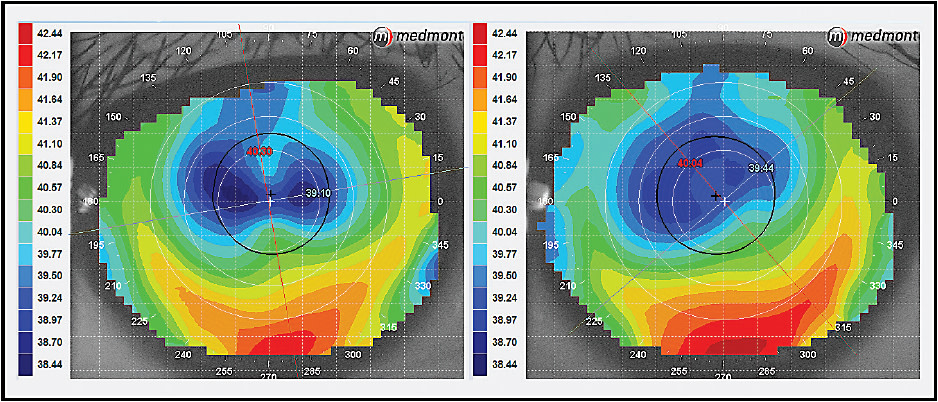
Figure 1. Axial topographies of our patient, who underwent bilateral LASIK in 2003.
He had researched orthokeratology as a possible means to stabilize and improve his vision. This patient was highly motivated to improve his vision and reduce the dependency on glasses and soft contact lens wear throughout the day.
Fitting Considerations
Fitting a post-PRK or post-LASIK patient with orthokeratology involves three straightforward fitting considerations.
Step 1 Choose a diagnostic lens from your standard orthokeratology lens system. In our case, we measured the sagittal depth of the cornea with the Medmont E300 (Medmont International Pty Ltd) corneal topographer, then added 10 microns of fluid allowance between the lens and cornea. Next, we selected the closest sagittal depth trial lens from our fitting set. If your topographer does not allow for the measurement of sagittal depth or your trial lenses are not categorized in terms of height, then choose the initial lens based on the pre-surgical K-readings and your orthokeratology lens nomogram. If none of the options above are available to you, start with the median lens in your diagnostic set.
Step 2 Evaluate the initial lens for centration, comfort, and peripheral alignment. If one or more of the criteria cannot be met, place the next steeper or flatter diagnostic lens on the eye until an acceptable peripheral relationship is achieved. The goal is to find a lens from the trial or inventory set whose periphery will center the required treatment within the pupil (Figure 2). Once you arrive at a lens with the appropriate periphery, the specifications of the outer zones are clearly understood.
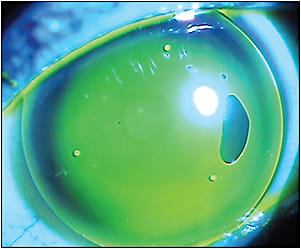
Figure 2. This trial lens exhibits good centration, peripheral alignment, and reasonable initial comfort. Although the center shows excessive apical clearance, the goal is to find a diagnostic lens with the correct peripheral relationship as a first step. Next, the apical clearance will be adjusted in the custom lens order to target the myopia reduction.
Step 3 Evaluate the apical clearance of the lens. To achieve the hydraulic force required to compress central epithelial tissue, the lens should be approximately 5 to 10 microns away from the corneal apex. Estimate the change in base curve required to lift or drop the center to create the orthokeratology fluorescein pattern customary in a normal prolate eye fit. This step requires “guesstimation” rather than calculation and has the greatest potential for error. However, mathematically, a base curve change of 0.10mm in an orthokeratology lens creates approximately 6 to 8 microns of apical clearance adjustment. Therefore, the minimal base curve alteration is approximately 0.15mm to create a measurable change in the central fluorescein pattern. Another approach is to alter the reverse curve radius by 0.12mm to 0.13mm, which creates a 10-micron adjustment in apical clearance. As you would expect, the apical clearance is the zone most likely to require refinement.
Once a patient’s custom lens is ordered, evaluate the fit prior to dispensing for overnight wear. Ensure that the lens appears to center adequately in the open-eye environment and that the apical clearance calculation produces a fluorescein pattern with near touch in the center (Figure 3). This should be surrounded by a reservoir of fluid to create the myopia reduction. Beyond the concentric ring of vault should be a wide landing or alignment zone with the peripheral cornea. Lastly, a healthy edge lift should be seen 360º around, which should present as a band of fluorescein approximately 0.5mm wide.
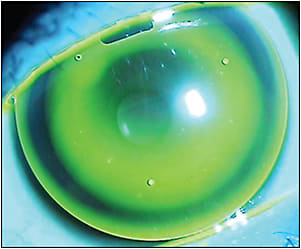
Figure 3. The trial lens base curve was altered to reduce the apical clearance in this custom lens and produce a pattern similar to a conventional orthokeratology fluorescein presentation. Evaluating from the outside in, this lens exhibits a healthy edge lift, good peripheral alignment, a concentric reservoir of fluid, and an apex close to the central cornea but not touching.
Following overnight wear, perform corneal topography and look for a centered bull’s-eye response that is no different from traditional orthokeratology cases. If a “smiley face” results, tighten the alignment zone to bring the lens down onto center. If the outcome is a “frowny face” topographical response, then loosen the alignment zone to bring the lens up. If the centration is acceptable but the effect results in a refractive under-correction, flatten the base curve only. Conversely, if an over-correction results, steepen the base curve to reduce the effect. You will find your laboratory consultants very helpful for these and other adjustments.
Our patient’s topographically measured sagittal depth indicated that he required a 9.10mm BE Retainer (Bausch + Lomb Vision Shaping Treatment design) trial lens for the right eye and a 9.00mm for the left eye. On initial evaluation, the diagnostic lenses were too flat and required much steeper base curves. It was determined that the 8.85mm trial lenses in both eyes provided alignment, centration, acceptable comfort, and a healthy edge lift. However, the apical clearance for both eyes was excessively high and would not have produced much, if any, myopia reduction. It was estimated that both trial lenses should have the sagittal depth reduced by 30 microns. Using the same zone parameters for each trial lens, the base curve of the custom lens was flattened by 0.40mm to lower the sagittal depth approximately 30 microns. In other words, the trial and custom parameters were identical with the exception of the base curve being altered.
Following one night of custom lens wear, the patient exhibited well-centered bull’s-eye topographies in both eyes and a residual Rx of right eye −1.00 −0.50 x 180 and left eye −1.25 −0.50 x 20. After one month of overnight wear, an additional modification was made resulting in a second set of custom lenses with a base curve 0.20mm flatter than the first custom lenses. The refraction after 12 nights of wear was right eye −0.25 −0.75 x 5 and left eye −1.00 −0.25 x 50. Following an additional two weeks of overnight wear in the same lenses, the refraction improved to plano −0.50 x 180 in the right eye and −0.25DS in the left eye. The BCVA was 20/20 in both eyes at all follow-up visits, and our patient has been successfully wearing the second set of custom lenses nightly for the past two years. He is very satisfied with the level of uncorrected vision throughout the day and with the overall stability of the refractive outcome.
Guidelines for Achieving Success
The following are guidelines and necessities for achieving success in orthokeratology on post-PRK or post-LASIK eyes:
• Mild myopia (< −2.00D)
• Mild astigmatism < −1.00D)
• Access to an orthokeratology diagnostic set or inventory system
• A corneal topographer
Determine which diagnostic lens will achieve optimal centration, peripheral alignment, and comfort. Adjust the apical clearance up or down to moderate the refractive outcome.
Lastly, consider that this type of fit will involve more office visits and lenses compared to a traditional orthokeratology treatment on a non-surgical eye. Be sure to charge appropriately for your chair time, and protect yourself with an informed consent and a healthy cancellation policy. Additionally, your fees should reflect the significant investment in tools (topographer and diagnostic sets), not to mention the clinical expertise required for this specialty contact lens fit.
Conclusion
Fitting post-refractive surgery eyes with orthokeratology lenses is not an easy endeavor. It requires practitioners to match a complex geometry with a highly specialized custom lens. However, it is possible to provide correction for these motivated patients who have mild degrees of residual refractive error. Armed with a few simple fitting considerations, successful outcomes are possible for post-refractive surgery patients desiring freedom from conventional contact lens and spectacle wear. CLS
For references, please visit www.clspectrum.com/references and click on document #246.

| Randy Kojima is a clinical research and development director for Precision Technology Services and a research scientist and clinical instructor at the Pacific University College of Optometry. He is a shareholder in Precision Technology and Cardinal Contact Lens and is an advisor to Medmont International. |

| Dr. Ho has a Doctor of Optometry from the University of Waterloo and a PhD in Neuroscience from the University of British Columbia. Her clinical practice in Vancouver, BC, focuses on specialty contact lens fitting and pediatric care. As a research associate, she has been involved in both independent research and clinical trials with the departments of Ophthalmology at the University of British Columbia and British Columbia’s Children’s Hospital. |